The Epworth Sleepiness Scale: Test Your Daytime Sleepiness
For years before I was diagnosed with severe obstructive sleep apnea, I lived inside a kind of low grade fog. Not the sort of tiredness that resolves with a long weekend or an extra coffee. The other kind. The kind where your brain pulls its weight grudgingly all day, where reading two paragraphs of a book turns into reading the same paragraph four times, where a quiet meeting after lunch becomes a fight to keep your eyes open. I assumed that was just what being a busy adult felt like.
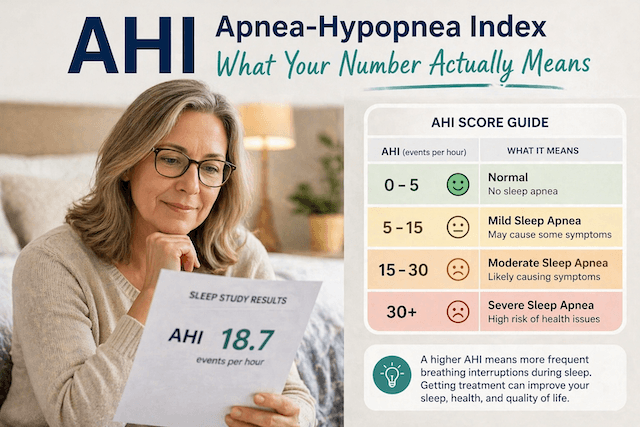
It wasn’t. It turned out my AHI was 51 (you can read more about what AHI means here), which placed me firmly in the severe category. My wife was the one who finally pushed me toward a sleep study, and the diagnosis explained more than a decade of feeling like I was running my life in low gear.
What I didn’t know back then is that an eight-question survey, taking less than three minutes, can flag exactly the kind of daytime sleepiness I was carrying around. It’s called the Epworth Sleepiness Scale, and it has been one of the most widely used screening tools in sleep medicine since 1991.
I’m a software guy by training, not a doctor. I write about this because I lived through the years that lead up to a diagnosis, and I have worn a CPAP every night for the better part of a decade since. Everything below is research and personal experience. None of it replaces a real conversation with a real clinician.
What the Epworth Sleepiness Scale Actually Measures
The Epworth Sleepiness Scale (ESS) was developed by Dr. Murray Johns at Epworth Hospital in Melbourne, Australia, and first published in the journal Sleep in 1991. (Yes, an Australian invention. As someone living in Western Australia, I will claim that one for the home team.) Johns wanted a simple, repeatable way to put a number on something that sleep doctors had previously been forced to assess by feel: how much of an unmet need for sleep a patient is carrying around during their waking hours.
The scale doesn’t measure how tired you feel right this minute. That’s a different thing, and it’s worth pausing on. Fatigue is the heaviness you notice after a long workout or a stressful week. The ESS measures something narrower and arguably more useful, which Johns called average sleep propensity: how likely you are to actually doze off, not just feel tired, in a range of normal everyday situations.
That’s why the questions are framed the way they are. They don’t ask “how exhausted are you” or “do you struggle to concentrate.” They ask, scenario by scenario, how likely you are to fall asleep. Sitting and reading. Watching TV. Sitting in traffic. Lying down to rest in the afternoon. Each scenario gets a score from 0 (would never doze) to 3 (high chance of dozing). The total runs from 0 to 24.
The reason this distinction matters is that plenty of people with sleep apnea will tell you they are not particularly tired. They have been dragging this baseline around for so long that it has become normal. But ask them whether they would fall asleep in front of the TV after dinner, or whether they have caught themselves nodding off as a passenger on a long drive, and the answer changes. The ESS catches that gap.
Why These Eight Scenarios
Johns picked the eight situations carefully. They span what sleep researchers call somnificity, which is the tendency of a given activity to push you toward sleep. Lying down to rest in the afternoon is high somnificity. Sitting and talking to someone is low. Sitting in traffic is somewhere in between. By spreading the scenarios across that spectrum, the scale gives a more reliable picture of average sleep propensity than any one situation could on its own.
A healthy adult with no underlying sleep disorder will typically score 0 or close to it for an active scenario like holding a conversation, but might legitimately score 1 or 2 for lying down in the afternoon. That’s normal human biology. What raises a flag is a high total score, especially when the higher numbers cluster on the more active scenarios. Dozing off mid-conversation or while stopped in traffic is a different signal from drifting off during a quiet rest after lunch.
The ESS doesn’t ask you to remember a single bad night, and it doesn’t ask how you feel today. It asks about your usual way of life in recent times. That phrasing is deliberate. It’s trying to surface the steady-state pattern, not catch you on an off day.
Take the Test
Take a moment, answer all eight as honestly as you can, and total your score. Be careful not to underestimate. People who have lived with daytime sleepiness for years often think their tiredness is simply how everyone feels, and they end up under-rating their dozing tendency.
Note: The Epworth Sleepiness Scale is a screening tool, not a diagnosis.
How to Read Your Score
The total runs from 0 to 24. Higher numbers mean a higher tendency to doze off in the situations the questionnaire describes. Here is how the score is generally interpreted today, in line with the bands used by the official ESS website and most current sleep medicine sources.
A score of 0 to 10 sits inside the normal range. That’s the same range that healthy adults without a sleep disorder typically fall into. It does not mean you have nothing going on, but it does mean the scale isn’t picking up an obvious sleep propensity problem.
A score of 11 or 12 indicates mild excessive daytime sleepiness. This is the band where I would start paying real attention, especially if you also snore, your partner has noticed pauses in your breathing at night, or you wake up unrefreshed.
A score of 13 to 15 indicates moderate to excessive daytime sleepiness. That’s a meaningful enough signal that a conversation with a doctor is warranted. Several conditions can drive a score into this range, sleep apnea being one of the most common.
A score of 16 to 24 indicates severe excessive daytime sleepiness. At this end of the scale, the chances that something significant is going on with your sleep are high, and a sleep study should be on the table sooner rather than later. This is also the range where drowsy driving becomes a serious safety issue.
When I eventually went through a sleep study, my own ESS came in well above the normal range, and the lab confirmed what my body had been trying to tell me for years. The number itself didn’t diagnose anything. What it did was give my doctor concrete evidence to push for a proper test, instead of leaving me with another vague “you should sleep more” conversation.
A small but important note: a low score does not rule out sleep apnea. The original validation work, which you can read in Johns’ 1991 paper on PubMed, found that ESS scores tend to be higher in patients with obstructive sleep apnea than in healthy controls, but plenty of people with confirmed apnea score in the normal range. If you snore, gasp, or have a partner watching you stop breathing in your sleep, please don’t let a low ESS score talk you out of a sleep study.
Why High Daytime Sleepiness Is a Big Deal
It’s tempting to file daytime sleepiness under “minor inconvenience.” Coffee, get on with your day, move along. But the research on excessive daytime sleepiness is sobering. People who score in the higher ranges of the ESS have measurably elevated risks of motor vehicle accidents and workplace incidents. Drowsy driving in particular is a serious public health issue, and the kind of dozing the ESS picks up is precisely the kind that gets people into trouble behind the wheel.
There’s also the cumulative effect on the rest of life. Years of unrecognized sleep fragmentation chip away at memory, mood, cognitive performance, and patience. I look back at the decade before my diagnosis and recognize, with the benefit of hindsight, a steady tax on my work, my relationships, and my general capacity to be present. None of that registered as a problem at the time. It just felt like adulthood. It wasn’t.
If you want a fuller picture of how untreated sleep apnea presents, my overview of sleep apnea symptoms lays out what to look for beyond just feeling tired. The ESS catches one piece of a larger pattern.
What the Epworth Sleepiness Scale Doesn’t Measure
The ESS is genuinely useful, but it has limits, and it’s worth being honest about them.
It is subjective. You’re scoring yourself, which means your answers are colored by how good you are at noticing your own dozing. People who have lived with severe daytime sleepiness for years often score themselves more conservatively than they should, because their internal calibration of “normal” has drifted.
It does not measure your breathing, your oxygen levels, or your brain activity during sleep. It cannot count apneas. For that, you need a sleep study, either a home test or an in-lab polysomnogram.
It is best validated for obstructive sleep apnea, narcolepsy, and idiopathic hypersomnia. It is less reliable for central sleep apnea, insomnia, and other conditions where the dominant symptom isn’t dozing during passive activities.
Because of those limits, sleep clinicians often pair the ESS with a second screening tool. The most common companion is the STOP-BANG questionnaire, which adds physical risk factors like neck circumference and blood pressure to the picture. If you’re trying to get a fuller pre-clinical read on your situation, doing both is more informative than doing either one alone. I have a separate piece on the STOP-BANG score and how to interpret it if you want to take that next step.
Using the ESS to Track Treatment
One of the more practical uses of the ESS, and the one I think gets undersold, is as a before and after measurement. If you start CPAP therapy and it’s working, your ESS score should drop. The original Johns research and several follow-up studies confirmed that successful CPAP treatment in patients with obstructive sleep apnea is reflected in a measurable decrease in ESS scores. It’s one of the cleanest subjective signals of “this is working.”
For me, the difference was clear within the first couple of months on my ResMed AirSense 10. The fog lifted in a way I hadn’t expected. Long drives became less hazardous. Afternoon meetings stopped feeling like a battle. I didn’t formally retake the ESS at the time, but in retrospect, I wish I had, just to have the number on paper. If you’re starting CPAP now, I’d suggest taking the test on day one and again around the three-month mark. It gives you a concrete, comparable data point to set alongside your machine’s reported AHI.
For more on what to look at in your CPAP data once you’re up and running, my piece on interpreting your CPAP data covers what’s actually worth tracking.
What to Do If Your Score Is High
Don’t panic. The ESS is a screening tool, not a diagnosis, and a high score has more than one possible cause. Sleep apnea is statistically the most common, but not the only one.
Start with your primary care doctor, ideally taking your score and a brief description of your symptoms with you. Mention any snoring, witnessed apneas, morning headaches, or unrefreshing sleep. If your doctor agrees the picture is suggestive, the next step is a sleep study. These come in two forms: a home sleep apnea test, which is convenient and increasingly common for suspected obstructive sleep apnea, or an in-lab polysomnogram, which captures more data and is the gold standard for harder cases.
I have written a fuller walkthrough of home sleep apnea tests and the diagnosis process if you want to know what to expect.
The thing I would most want my pre-diagnosis self to hear is this: don’t sit on the score for years the way I sat on the symptoms. The cost of investigating is small. The cost of ignoring is high.
Final Thoughts
Eight questions. Three minutes. A score from zero to twenty-four. That’s all the Epworth Sleepiness Scale is. It will not tell you whether you have sleep apnea, and it will not tell you what to do next. What it will do is give you a concrete number for something you might have been carrying around for years without examining: how often, and how easily, you fall asleep when you’re not supposed to.
If your score is in the normal range, that’s useful information. If it isn’t, you now have a piece of evidence to take to a doctor, instead of trying to describe a vague feeling of being tired all the time. Either way, you have spent three minutes well.
If you’re new to all of this, my beginner’s guide to sleep apnea is a sensible next stop. And if you have already started CPAP therapy and the early going is rough, you’re not alone. I have written separately about overcoming CPAP anxiety in those first few weeks.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).