Shrinking Rather Than Removing the Tonsils: Less Invasive?
For a long time, taking the tonsils out was almost automatic. Sore throats, snoring, trouble sleeping, and out they came. For generations of children it was close to a rite of passage, usually remembered afterward for the bowls of ice cream more than the surgery itself.
Medicine has moved on, and so has our understanding of what the tonsils actually do. A growing number of ear, nose and throat specialists now question whether full removal is always the right call. Instead of taking the tonsils out completely, many of them offer something gentler: shrinking them.
That shift matters for anyone weighing surgery for snoring or sleep apnea, whether for themselves or for a child. Before I go any further, the usual and important caveat. My background is in computer science, not medicine. I have lived with severe obstructive sleep apnea for more than a decade, and I write as a patient who has spent a long time reading the research, not as a clinician. Nothing here is medical advice. Talk to your own doctor about your situation.
If you are still working out whether your tonsils are part of the problem, my piece on whether enlarged tonsils can cause snoring is a good place to start.
What the tonsils are, and why they matter
The tonsils are two small pads of soft tissue at the back of the throat. They are part of the immune system, among the body’s earlier lines of defense against the bacteria and viruses that arrive through the mouth and nose. In childhood especially, they do real work helping the immune system learn what it is up against.
For some people, though, and again especially for children, those small glands become a big problem. When they grow large enough, they can crowd the airway during sleep, or they can become infected again and again. Either situation can push a family toward surgery. Large tonsils are one of the more common reasons a child develops obstructive sleep apnea, and they can contribute in adults too.
Here is the trade-off that drives the newer thinking. Removing the tonsils means removing immune tissue, and it exposes the muscle bed underneath, which is where most of the pain and bleeding risk after surgery comes from. Reducing their size rather than cutting them out entirely is an attempt to relieve the obstruction while leaving that protective layer in place.
The idea behind shrinking instead of removing
Tonsil reduction, also called partial tonsillectomy or tonsillotomy, removes most of the tonsil but deliberately leaves a thin rim of tissue behind. That remaining cushion covers the nerves and blood vessels underneath, which is the main reason recovery tends to be faster and less painful than a full tonsillectomy.
Surgeons reach that result in a few different ways. Coblation uses low-temperature radiofrequency energy to break down tissue gently rather than burning through it. A Cochrane review hosted by the National Library of Medicine has examined how coblation compares with other surgical techniques. Laser reduction vaporizes excess tissue with focused light. Intracapsular tonsillectomy removes the bulk of the tonsil while leaving the outer capsule intact to protect nearby structures. Radiofrequency ablation works from inside the tissue, heating it so that it shrinks over a period of weeks.
Most of these are outpatient procedures, and in many cases, especially with children, patients are back to normal life within a few days rather than a couple of weeks. For a wider look at how these approaches sit alongside more involved operations, see my overview of sleep apnea surgery options.
Does it actually work?
The strongest evidence so far comes from children. A 10-year study from Flinders University in Australia followed more than 600 children who had either a full tonsillectomy or a partial reduction between 2008 and 2018.
The children who had the reduction returned to normal activity in about 4.6 days on average, compared with 11.1 days after full removal. They were roughly three times less likely to have any bleeding, and about eight times less likely to have a serious bleed that sent them back to hospital. Just as important, the improvement in breathing and sleep was similar in both groups.
That last point is the one that changes the conversation. Even with a rim of tonsil left in place, the relief from snoring and obstructive sleep apnea held up. If the goal is to open the airway, the data suggest you may not need to remove every last piece of tissue to get there.
Children’s airways are not adult airways, though, so the pediatric picture is worth understanding in its own right. If you are reading this as a parent, how to tell whether your child has sleep apnea and my broader piece on sleep apnea in children go deeper.
Who it tends to suit
Tonsil reduction is not the right answer for everyone, and a good surgeon will say so. It tends to fit best when the tonsils are clearly enlarged and driving mild or moderate sleep apnea or heavy snoring, when infections are occasional rather than constant, and when the patient or family is understandably worried about pain, bleeding, or time away from school or work. Adults who want symptom relief with less surgical trauma can be reasonable candidates as well.
It is a poorer fit in other situations. Repeated severe tonsillitis, meaning several serious infections a year, is one of the classic reasons to remove the tonsils entirely. Tonsil abscesses, any suspicion of cancer, tonsils so large they nearly block the airway on their own, and cases where tissue needs to be removed for a biopsy all point toward full removal rather than reduction.
To work out which group a given person falls into, specialists lean on a sleep study, a physical exam of the throat, and the medical history. A simple airway exam such as the Mallampati score helps a clinician judge how crowded the throat really is. If your ENT has raised a more involved operation like uvulopalatopharyngoplasty, it is worth understanding how that differs, since the tonsils are often part of that procedure too.
Reduction versus full removal
Set side by side, the differences are fairly consistent. Reduction usually means less pain during recovery, a faster return to normal activity, and a lower risk of bleeding, and it keeps some immune tissue in place. Its main drawback is that, in a small number of cases, regrowth can mean a second procedure later on. Full removal is more painful and slower to recover from, with a higher risk of late bleeding, and it takes all the tonsil tissue with it. In return, it is usually a one-time operation and remains the right choice when recurring infection, rather than airway obstruction, is the real problem.
For many families, the gentler healing and the lower complication risk are what tip the decision toward reduction. For others, particularly where infection is the main issue, full removal still makes more sense. There is no single correct answer here, only the answer that fits the actual problem.
What about adults with sleep apnea?
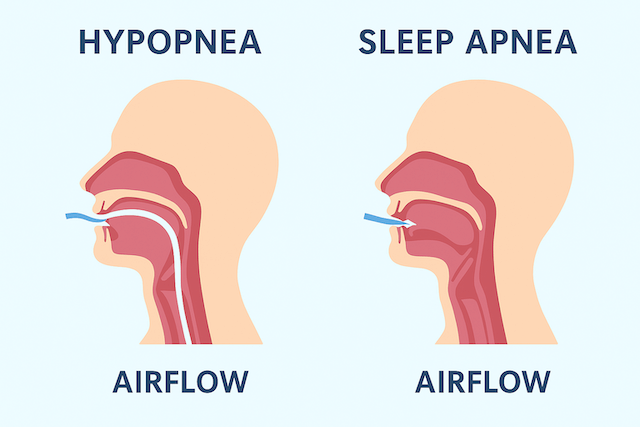
Most of the research sits with children, but adults whose sleep apnea is driven by large tonsils can benefit too. A systematic review and meta analysis published in The Laryngoscope pulled together 17 studies of adults who had tonsillectomy alone for obstructive sleep apnea. Across those patients, the apnea hypopnea index, the AHI score used to grade severity, fell by roughly 65 percent on average.
The catch, and it is a big one, is that success depends heavily on anatomy and on how severe the apnea was to begin with. In that same analysis, adults who started with mild to moderate sleep apnea did extremely well, while those who started with severe apnea improved far less reliably. That distinction is personal for me. My own AHI was 51 at diagnosis, which sits firmly in the severe range, and it is a clear illustration of why surgery on a single site is rarely a complete fix once apnea is that advanced. When the obstruction comes from the tongue, the soft palate, or the nose as much as from the tonsils, shrinking the tonsils alone will not solve it.
That is why thoughtful ENT surgeons often recommend a test called drug-induced sleep endoscopy, or DISE, before operating on an adult. Under light sedation that mimics sleep, the surgeon watches where the airway actually collapses, so the operation can target the real bottleneck rather than the most obvious one. It is one more reason to work with a team that takes the time to map your particular airway rather than reaching for the same procedure for everyone.
If you are exploring surgery at all, it helps to know what else is on the menu, from oral appliances like the ones I cover in my guide to sleep apnea mouth guards to nerve stimulation approaches such as Inspire therapy and hypoglossal nerve stimulation. Weight and overall airway anatomy matter as well, which is something I get into in my piece on CPAP therapy and weight loss.
Where I landed, and why
I want to be clear about my own path, because it shapes how I read all of this. I did not have tonsil surgery. When I was diagnosed with severe sleep apnea, I went down the CPAP road, and more than a decade later I am still on it. As a lifelong mouth breather I use a full face mask, and the therapy has done its job.
So I am not writing this as someone who shrank his tonsils and woke up cured. I am writing as a patient who, once diagnosed, wanted to understand the whole landscape of options, including the ones I did not take. Tonsil reduction was one of those. When I first came across it, I had the same reaction a lot of people do, which is some version of, why isn’t this talked about more? It will not be the answer for everyone, and for severe apnea like mine it is rarely the whole answer, but for the right person it is a genuinely gentler road than the operation their parents or grandparents would have faced.
If surgery turns out not to be your path either, my honest look at whether sleep apnea can ever truly be cured covers what treatment can and cannot do.
Questions worth asking your ENT
If you are weighing tonsil reduction, or a full tonsillectomy, a few questions tend to cut through the uncertainty. Ask which technique the surgeon uses and why, whether coblation, intracapsular, or laser. Ask about their own complication rate for bleeding and infection rather than the textbook figures. Ask, specifically, whether this is likely to help your sleep apnea symptoms given your particular airway, and whether they perform or recommend DISE to confirm where the blockage actually is. Ask what recovery will realistically look like for you or your child, and whether there are non surgical options worth trying first.
A good surgeon will not rush any of that. They will walk you through the risks, the alternatives, and the likely outcome based on your history, not a generic script.
Common questions
Do tonsils grow back after a reduction? They can regrow a little, particularly in younger children, but full regrowth is uncommon, and most people never need a second operation.
Is it really less painful than full removal? For most patients, yes. The studies consistently show less pain after partial removal, and many people manage on over-the-counter pain relief rather than prescription medication.
Does it work for sleep apnea? When the apnea is being driven by enlarged tonsils, it can work well, in both children and adults. When the obstruction is coming from elsewhere in the airway, reducing the tonsils alone is unlikely to fix it.
Is it covered by insurance? Often, especially when it is medically necessary, and many plans treat it much like a traditional tonsillectomy. Coverage still varies, so confirm the details with your own provider.
Can adults have it done? Yes. It is more common in children, but adults with enlarged tonsils can be good candidates, particularly when the main goals are opening the airway and reducing snoring.
The bottom line
If someone you love is struggling to breathe at night, or dealing with repeated sore throats, tonsil reduction is worth knowing about. It is not about avoiding treatment. It is about choosing the option that fits the problem, with the least collateral damage along the way.
The sensible first step is a conversation with an ENT about whether intracapsular tonsillectomy, coblation, or partial reduction makes sense in your case, and how they decide which technique suits which patient. If sleep apnea is what brought you here, understanding how the condition is diagnosed is a good companion read.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).