Do I Have Sleep Apnea? How to Recognize the Signs and Get Help
I’ll never forget the morning my wife sat me down at the kitchen table and told me she was genuinely worried I might not wake up one night.

We’d been together for six years at that point. For most of that time, she’d complained about my snoring. Loud, persistent snoring that rattled the windows and drove her to sleep in the guest room more nights than I care to admit. I brushed it off. “I’ve always been a heavy snorer,” I told her. “It’s no big deal.”
But that morning was different. Her voice shook as she described watching me stop breathing during the night. Not once or twice, but repeatedly. She’d count the seconds, holding her breath with me, until I’d suddenly gasp and jerk awake just enough to start the cycle again. She told me I’d literally turn purple.
I finally listened. Within two weeks, I had a home sleep test scheduled.
The results hit me like a freight train. My Apnea Hypopnea Index (AHI) came back between 51 and 58. Severe obstructive sleep apnea. During the worst episodes, my oxygen levels dropped to 78%. For context, anything below 90% is considered medically concerning.
I was suffocating hundreds of times every night and had no idea.
If you’re reading this and wondering “Do I have sleep apnea?” then you’re already ahead of where I was. You’re paying attention to the warning signs. Maybe your partner noticed something. Maybe you’re exhausted despite sleeping eight hours. Maybe the morning headaches are getting worse.
Whatever brought you here, the fact that you’re asking the question means it’s time to get answers. Let me share what I learned through my diagnosis journey and over a decade of CPAP therapy since.
Sleep Apnea Quiz: Try the Epworth Sleepiness Scale
Before we dive deeper, let’s start with a simple screening tool that doctors use all the time: the Epworth Sleepiness Scale (ESS). This questionnaire measures your likelihood of dozing off in everyday situations. High scores can be a red flag for sleep apnea, though they’re not diagnostic on their own.
The ESS was developed by Dr. Murray Johns at Epworth Hospital in Melbourne, Australia in 1991. Research shows it has good validity for identifying excessive daytime sleepiness, one of the hallmark symptoms of sleep apnea. When researchers compared ESS scores to sleep study results, they found that people with severe sleep apnea averaged scores around 14.3, compared to 7.6 for people without sleep disorders.
Studies also show an interesting wrinkle: when bed partners fill out the ESS for their spouse, the scores are often significantly higher than what patients report themselves. In one study, 73% of people underestimated their own sleepiness compared to what their partners observed. Your partner might see what you’ve been missing.
Take a couple of minutes to complete this honestly:
Try the Epworth Sleepiness Scale
Answer honestly and think about your usual way of life in recent times, not just how you feel today. It only takes a couple of minutes.
Note: The Epworth Sleepiness Scale is a screening tool, not a diagnosis. If your score is high, consider discussing a home sleep apnea test with your doctor. For more details on interpreting your results, check out my complete guide to the Epworth Sleepiness Scale.
Recognizing the Warning Signs You May Have Sleep Apnea
When I look back now, the signs were everywhere. I just didn’t know what I was looking at.
The crushing fatigue was the worst part. I’d sleep nine hours and wake up feeling like I’d run a marathon. By mid afternoon, I could barely keep my eyes open at my desk. I’d catch myself nodding off in meetings, during phone calls, even while driving on the highway. That last one terrified me once I understood what was happening.
The morning headaches started gradually. At first, just occasional. Then daily. Then they evolved into full migraines that would knock me out for hours. I tried every painkiller, adjusted my pillows, changed my mattress. Nothing helped because I was treating the symptom, not the cause.
Here are the most common signs of sleep apnea, based both on research and my experience:
Nighttime Symptoms:
- Loud, chronic snoring that disturbs your partner
- Gasping, choking, or snorting sounds during sleep
- Witnessed breathing pauses or cessations
- Frequent nighttime urination (nocturia)
- Restless sleep with frequent position changes
- Night sweats unrelated to room temperature
- Waking with a dry mouth or parched throat
Daytime Symptoms:
- Excessive daytime sleepiness despite adequate time in bed
- Morning headaches that fade within a few hours
- Difficulty concentrating or focusing on tasks
- Memory problems and brain fog
- Irritability, mood changes, or depression
- Decreased interest in activities you once enjoyed
- Falling asleep during quiet activities like reading or watching TV
Research confirms what many of us experience. One study found that morning headaches occur in up to 74% of people with obstructive sleep apnea. The headaches result from carbon dioxide retention and oxygen deprivation during the night, causing blood vessels in the brain to dilate.
Not everyone with sleep apnea experiences excessive daytime sleepiness. Studies show that only 15% to 50% of people with sleep apnea in the general population report feeling sleepy during the day. This is why many cases go undiagnosed for years. You can have severe sleep apnea and feel relatively alert during the day, especially if you’ve adapted to chronic poor sleep over many years.
My wife’s observation about my breathing pauses was the critical clue. Research shows that bed partner reports of witnessed apneas are one of the strongest predictors of sleep apnea, more reliable than self-reported symptoms. If someone who sleeps near you has noticed you stop breathing, take that seriously.
Do I Have Sleep Apnea If I Just Snore?
This was my first question when my wife suggested I get tested. “Doesn’t everyone who snores have sleep apnea? Isn’t it just loud breathing?”
The answer is no. Not everyone who snores has sleep apnea, and not everyone with sleep apnea snores loudly.
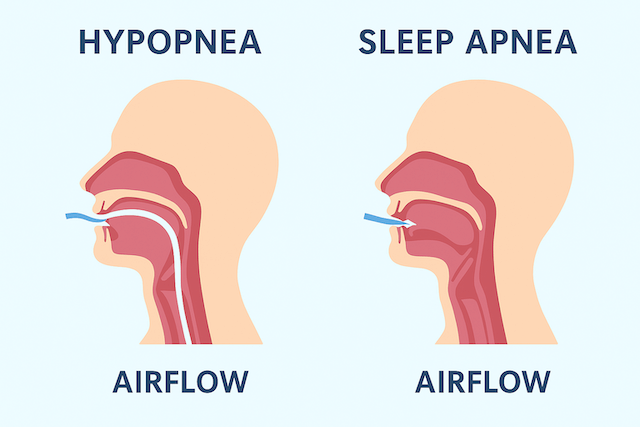
Snoring happens when airflow causes the tissues in your throat to vibrate during sleep. It’s common and affects roughly 40% of adult men and 24% of adult women. Most snoring is benign, though annoying to whoever has to listen to it.
Sleep apnea is different. With sleep apnea, your airway doesn’t just vibrate. It collapses, either partially or completely, cutting off your oxygen supply. Your body responds with a stress reaction, jolting you partially awake to restart breathing. This can happen hundreds of times per night.
The key differences to watch for:
Benign Snoring:
- Consistent snoring throughout the night
- No gasping or choking sounds
- No observed breathing pauses
- Generally feels rested in the morning
- Snoring may worsen with alcohol or sleeping on back
Sleep Apnea:
- Snoring interrupted by periods of silence (the pauses)
- Loud gasps or choking sounds when breathing resumes
- Partner witnesses you stop breathing
- Wake up exhausted regardless of sleep duration
- Morning headaches, dry mouth, sore throat
- Excessive daytime sleepiness
I was firmly in the second category. My wife described my breathing pattern like clockwork: loud snoring that would suddenly stop, complete silence for 20 to 30 seconds while I turned purple, then a desperate gasp as I’d partially wake to breathe again. Rinse and repeat, all night long.
If your snoring follows this pattern, or if you have other concerning symptoms, you need to get tested. The difference between simple snoring and sleep apnea is the difference between an annoyance and a life threatening medical condition.
Understanding the Types of Sleep Apnea
When I was first diagnosed, I thought sleep apnea was sleep apnea. One condition, one treatment. I quickly learned it’s more nuanced than that.
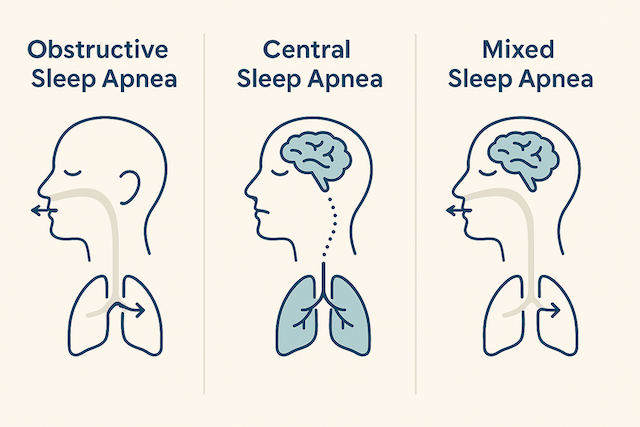
There are three main types:
Obstructive Sleep Apnea (OSA)
This is what I have, and it’s the most common type, accounting for roughly 84% of all sleep apnea cases. OSA happens when your airway physically collapses or becomes blocked during sleep.
The usual culprits include:
- Excess weight that adds tissue around the airway
- Naturally narrow airways
- Large tonsils or tongue
- Jaw structure that positions your tongue too far back
- Nasal congestion or deviated septum
When you fall into deeper sleep, the muscles in your throat relax. In people with OSA, this relaxation allows the soft tissues to collapse inward, blocking airflow. Your diaphragm and chest muscles work harder to pull air through the blocked passage, but nothing gets through until your brain triggers a partial awakening to tighten those throat muscles again.
For a detailed explanation of OSA mechanics and risk factors, see my guide on obstructive sleep apnea.
Central Sleep Apnea (CSA)
Central sleep apnea is less common and works differently. With CSA, your airway stays open, but your brain fails to signal your breathing muscles to work. Essentially, your brain “forgets” to tell your body to breathe.
CSA often occurs in people with:
- Heart failure or stroke
- Neurological conditions
- Use of certain medications, particularly opioids
- High altitude
CSA requires different treatment than OSA, often involving specialized devices like ASV (Adaptive Servo Ventilation) machines rather than standard CPAP. Learn more in my article on central sleep apnea.
Complex or Mixed Sleep Apnea
Also called treatment emergent central sleep apnea, this condition starts as obstructive sleep apnea but develops central apnea patterns when treated with CPAP therapy. It affects about 15% of people diagnosed with OSA who start CPAP treatment.
I initially wondered if I had this because my early CPAP data showed some central events. My sleep doctor explained that occasional central events are normal as your body adjusts to therapy. True complex sleep apnea is persistent and requires adjustments to treatment.
Why Untreated Sleep Apnea Is Deadly Serious
When my doctor first explained my AHI of 51-58, he didn’t sugarcoat the risks. “This isn’t just about being tired,” he said. “This is about your long term survival.”
He was right. The research on untreated sleep apnea is sobering.
Cardiovascular Disease and Mortality
Sleep apnea puts tremendous strain on your cardiovascular system. Every time you stop breathing, your oxygen levels drop and your blood pressure spikes. Your sympathetic nervous system goes into fight or flight mode. This happens hundreds of times per night, night after night, year after year.
A landmark Australian study followed 400 community members for 14 years. People with moderate to severe sleep apnea had a 33% mortality rate compared to just 6.5% mortality in people without sleep apnea. The adjusted hazard ratio was 6.24, roughly equivalent to the mortality risk of being 17.5 years older or having blood pressure 29 mm Hg higher.
More recent research published in 2025 found that prolonged exposure to the intermittent oxygen drops characteristic of sleep apnea accelerates cardiovascular aging and significantly increases mortality risk. The study showed clear signs of accelerated cardiovascular aging, including increased blood pressure, impaired heart function, reduced vascular flexibility, and abnormalities in cardiac electrical activity.
Another Wisconsin Sleep Cohort study found that people with severe sleep apnea had three times the risk of dying from any cause compared to people without sleep apnea. When they excluded people using CPAP therapy from the analysis, the hazard ratio for cardiovascular mortality jumped from 2.9 to 5.2.
The message is clear: untreated sleep apnea dramatically increases your risk of heart attack, stroke, and premature death. But treatment with CPAP appears to reduce these risks substantially.
Metabolic Disease
Sleep apnea is strongly linked to type 2 diabetes and metabolic syndrome. The intermittent hypoxia (low oxygen levels) triggers insulin resistance and glucose metabolism problems.
Research shows that OSA is independently associated with increased risk of developing type 2 diabetes, even after controlling for obesity and other risk factors. The relationship is bidirectional: OSA can lead to diabetes, and diabetes can worsen OSA.
I noticed this personally. Before CPAP, my fasting blood glucose was creeping toward prediabetic levels. After six months on CPAP therapy, my numbers had normalized without any other changes to my diet or exercise.
Cognitive Decline and Mental Health
The brain fog I experienced before treatment wasn’t just in my head. Sleep apnea causes measurable cognitive impairment.
Studies show that untreated OSA is associated with:
- Impaired memory consolidation
- Reduced attention and concentration
- Slower reaction times
- Increased risk of depression and anxiety
- Higher risk of accidents and injuries
The good news? These cognitive effects are often reversible with treatment. Within weeks of starting CPAP, I felt like my brain had been rebooted. I could focus again. My memory improved. The constant mental fog lifted.
For more on this connection, see my article on CPAP therapy and brain fog.
Safety Risks
Falling asleep while driving was one of my biggest fears before diagnosis, and for good reason. Research shows that people with untreated sleep apnea have two to three times the risk of motor vehicle accidents compared to the general population.
The same elevated risk applies to workplace accidents. If you operate machinery, work at heights, or have any safety-critical job, undiagnosed sleep apnea puts both you and others at risk.
How Sleep Apnea Is Diagnosed
Once I accepted that I needed testing, the next question was: what kind of test?
There are two main diagnostic pathways: home sleep apnea testing and in-lab polysomnography. Here’s what you need to know about each.
Home Sleep Apnea Test (HSAT)
This is what I did, and it’s become the standard first step for most people with suspected OSA.
A home sleep apnea test uses a portable device that records your breathing patterns, oxygen levels, heart rate, and sometimes body position while you sleep in your own bed. You typically pick up the device from your doctor’s office or have it mailed to you, wear it for one or two nights, then return it for analysis.
What it measures:
- Airflow through your nose and mouth
- Breathing effort (chest and abdominal movement)
- Blood oxygen saturation
- Heart rate
- Snoring
- Body position
The device calculates your AHI (apneas and hypopneas per hour) and generates a report for your doctor to review.
Advantages:
- Sleep in your own bed in familiar surroundings
- More convenient and accessible
- Significantly less expensive than lab testing
- Usually covered by insurance for appropriate candidates
- Results typically available within a few days
Limitations:
- May underdiagnose mild sleep apnea
- Doesn’t measure actual sleep time (uses recording time instead)
- Can’t detect sleep stages or other sleep disorders
- May fail if sensors move or disconnect during the night
Research on HSAT accuracy is generally positive. The American Academy of Sleep Medicine endorses home sleep testing as an alternative to in-lab polysomnography for diagnosing OSA in adults with symptoms suggesting moderate to severe sleep apnea and no other significant medical conditions.
A 2018 validation study found that HSAT demonstrated good feasibility and sufficient accuracy compared to polysomnography, with acceptable night to night variability. The study concluded that HSAT is a viable alternative to PSG in appropriate patients.
I’ve written a comprehensive guide to help you understand the process: At Home Sleep Apnea Test: Everything You Need to Know.
One specific device I recommend is the WatchPAT One, an FDA-cleared single use home test that’s surprisingly accurate and incredibly easy to use.
In Lab Polysomnography (PSG)
This is the gold standard diagnostic test for sleep disorders. You spend the night in a sleep lab while technicians monitor you with extensive sensors.
What it measures:
- Everything the home test measures, plus:
- Brain waves (EEG) to determine sleep stages
- Eye movements (EOG) to detect REM sleep
- Muscle activity (EMG) in legs and jaw
- Continuous audio and video recording
When to choose lab testing:
- Home sleep test results are inconclusive
- You have other sleep disorders (insomnia, narcolepsy, parasomnias)
- Significant heart or lung disease
- Neurological conditions
- Central sleep apnea suspected
- Need for CPAP pressure titration during diagnosis
In lab testing provides the most comprehensive data, but it’s more expensive, less convenient, and some people struggle to sleep normally in the unfamiliar environment.
Understanding Your Results: AHI Explained
Whether you do home or lab testing, your results will include your Apnea Hypopnea Index (AHI). This number indicates the average number of breathing disruptions per hour of sleep.
AHI Classification:
- Normal: AHI less than 5
- Mild OSA: AHI 5 to 14
- Moderate OSA: AHI 15 to 29
- Severe OSA: AHI 30 or greater
My AHI of 51-58 placed me firmly in the severe category. I was stopping breathing, on average, once per minute all night long.
For a deeper dive into AHI scoring, interpretation, and what the numbers really mean, read my complete guide: AHI (Apnea Hypopnea Index): What Your Sleep Study Score Means.
Treatment Options When You Have Sleep Apnea
Getting diagnosed was scary. But it also meant I could finally do something about it.
Treatment options depend on the severity of your sleep apnea, the type (obstructive vs. central), and your individual circumstances. Here’s an overview of what’s available:
CPAP Therapy
Continuous Positive Airway Pressure (CPAP) is the gold standard treatment for moderate to severe OSA. The machine delivers pressurized air through a mask, creating enough pressure to keep your airway open throughout the night.
I’ve been using a ResMed AirSense 10 for over seven years (my previous machine lasted five years before this one).
During this time, I have only used a ResMed AirFit F20 full face mask.
I believe this therapy has added years to my lifespan.
The results were dramatic. Within the first week, my morning headaches disappeared. Within two weeks, my energy levels soared. Within a month, my wife said I was a different person, calmer, more patient, more engaged.
CPAP Quick Facts:
- Highly effective for OSA with AHI reduction of 80% or more
- Requires nightly use for benefits
- Adjustment period of days to weeks
- Various mask types available to fit your needs
- Learn more: Best CPAP Machines of 2025
I won’t lie, CPAP has a learning curve. The first few nights were rough. But the benefits so dramatically outweighed the initial discomfort that I stuck with it. For tips on making the adjustment easier, see my guide: How to Get Used to CPAP Therapy.
Oral Appliances
For mild to moderate OSA, or for people who can’t tolerate CPAP, custom oral appliances can be effective. These devices reposition your jaw or tongue to keep your airway open during sleep.
I haven’t used these personally, but many people in the sleep apnea community report good results, especially for mild cases. Learn more in my guide: Best Sleep Apnea Mouth Guards and Oral Appliances.
Lifestyle Modifications
These changes can reduce sleep apnea severity, though they’re rarely sufficient as standalone treatments for moderate to severe cases:
- Weight loss: Even a 10% reduction in body weight can significantly improve AHI
- Positional therapy: Sleeping on your side instead of your back reduces apnea frequency
- Avoid alcohol and sedatives: These relax throat muscles and worsen obstruction
- Treat nasal congestion: Clear nasal passages improve breathing
- Quit smoking: Reduces inflammation and fluid retention in upper airways
Read more: Positional Therapy for Sleep Apnea and Can You Reverse Sleep Apnea Naturally?
Surgical Options
Surgery may be considered when other treatments have failed or aren’t appropriate. Options include:
- UPPP (Uvulopalatopharyngoplasty): Removes excess tissue from the throat
- Hypoglossal nerve stimulation (Inspire): An Implanted device stimulates tongue muscle
- Jaw repositioning surgery: Moves jaw forward to enlarge airway
- Tonsillectomy or adenoidectomy: Removes enlarged tonsils/adenoids
Learn more: Sleep Apnea Surgery Options, Hypoglossal Nerve Stimulation, and Inspire Treatment for Sleep Apnea.
For a complete overview of all available treatments, see: Sleep Apnea Treatment: Complete Guide to Your Options.
Frequently Asked Questions
Q: Can sleep apnea go away on its own?
A: Sleep apnea rarely resolves without intervention. If your sleep apnea is caused by temporary factors like nasal congestion, enlarged tonsils in children, or recent weight gain, addressing those issues may reduce or eliminate symptoms. However, for most adults, sleep apnea is a chronic condition that requires ongoing treatment.
Q: How accurate is the Epworth Sleepiness Scale for diagnosing sleep apnea?
A: The ESS is a valuable screening tool but not diagnostic. Research shows it correlates with OSA severity, but correlation isn’t perfect. You can have severe sleep apnea with a normal ESS score, and you can have an elevated score without sleep apnea. The ESS should prompt further evaluation, not replace proper sleep testing.
Q: Should I get tested if I don’t feel sleepy during the day?
A: Yes, if you have other risk factors or symptoms. Many people with severe sleep apnea don’t experience excessive daytime sleepiness. Other symptoms like morning headaches, witnessed breathing pauses, frequent nighttime urination, or cardiovascular issues should prompt testing regardless of your daytime alertness.
Q: Is a home sleep test as accurate as a lab study?
A: For uncomplicated adults with symptoms suggesting moderate to severe OSA, home sleep tests are generally accurate. However, they may miss mild sleep apnea and can’t detect other sleep disorders. The American Academy of Sleep Medicine endorses home testing as an alternative to lab testing for appropriate candidates. If your home test is negative but symptoms persist, follow up with lab testing.
Q: Can children have sleep apnea?
A: Yes, and it’s more common than most people realize. Children’s sleep apnea often presents differently than adult sleep apnea, with symptoms like behavioral problems, bedwetting, mouth breathing, and poor growth. If you suspect your child has sleep apnea, see my guide: Sleep Apnea in Children: What Parents Need to Know.
Q: Will losing weight cure my sleep apnea?
A: Weight loss can significantly improve or even resolve sleep apnea in some people, particularly if excess weight was a primary contributing factor. However, sleep apnea has multiple causes, including anatomical factors that aren’t affected by weight. Many thin people have sleep apnea. Don’t skip testing and treatment while pursuing weight loss.
Q: How long does it take to feel better after starting treatment?
A: This varies. Some people feel dramatically better within days, like I did with my morning headaches. Others notice gradual improvements over weeks to months. Daytime sleepiness typically improves within 1-2 weeks. Cardiovascular benefits accrue over longer periods. The key is consistent use of whatever treatment you’re prescribed.
Take Action Now: Don’t Wait Like I Did
Looking back, I wish I’d listened to my wife sooner. I wish I’d paid attention to the warning signs years before I finally got tested. All those mornings waking up exhausted. All those afternoons fighting to stay awake. All those headaches and mood swings and moments of brain fog.
I was slowly suffocating myself hundreds of times every night and didn’t even know it.
If you’re reading this and recognizing yourself in these symptoms, please don’t wait. Don’t brush off your partner’s concerns. Don’t assume that feeling tired all the time is just normal aging or stress.
Take the Epworth Sleepiness Scale quiz above. Talk to your doctor about your symptoms. Get a sleep test, whether at home or in a lab.
Sleep apnea is one of the most common and most underdiagnosed medical conditions in the world. An estimated 90% of people with sleep apnea don’t know they have it. They’re walking around with a treatable condition that’s slowly damaging their heart, their brain, and their overall health.
You don’t have to be one of them.
Getting diagnosed was the first step. Starting CPAP therapy changed everything. The morning headaches and migraines that had plagued me for years vanished within weeks. My energy returned. My mood stabilized. My wife could sleep in our bed again without worrying I’d stop breathing in the middle of the night.
More importantly, I reduced my risk of heart attack, stroke, and premature death. I added years to my life and life to my years.
That’s what treatment can do. But first, you need to know if you have sleep apnea.
If you’re ready to take the next step, start here: At Home Sleep Apnea Test: Complete Guide or speak with your doctor about getting tested. Your future self will thank you.
References
- Johns, M.W. (1991). A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep, 14(6), 540-545. https://doi.org/10.1093/sleep/14.6.540
- Bhat, S., Upadhyay, H., DeBari, V.A., Ahmad, M., Polos, P.G., & Chokroverty, S. (2016). The utility of patient-completed and partner-completed Epworth Sleepiness Scale scores in the evaluation of obstructive sleep apnea. Sleep and Breathing, 20(4), 1347-1354. https://link.springer.com/article/10.1007/s11325-016-1362-0
- Goksan, B., Gunduz, A., Karadeniz, D., Agan, K., Tascilar, F.N., Tan, F., Purisa, S., & Erdag, E. (2009). Morning headache in sleep apnoea: clinical and polysomnographic evaluation and response to nasal continuous positive airway pressure. Cephalalgia, 29(6), 635-641. https://doi.org/10.1111/j.1468-2982.2008.01782.x
- Young, T., Peppard, P.E., & Gottlieb, D.J. (2002). Epidemiology of obstructive sleep apnea: a population health perspective. American Journal of Respiratory and Critical Care Medicine, 165(9), 1217-1239. https://www.atsjournals.org/doi/10.1164/rccm.2109080
- Marshall, N.S., Wong, K.K., Liu, P.Y., Cullen, S.R., Knuiman, M.W., & Grunstein, R.R. (2008). Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep, 31(8), 1079-1085. https://doi.org/10.5665/sleep/31.8.1079
- Badran, M., Puech, C., & Gozal, D. (2025). Prolonged intermittent hypoxia accelerates cardiovascular aging and mortality: insights from a murine model of OSA. npj Aging, 1, 4. https://www.nature.com/articles/s41514-025-00283-4
- Young, T., Finn, L., Peppard, P.E., Szklo-Coxe, M., Austin, D., Nieto, F.J., Stubbs, R., & Hla, K.M. (2008). Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep, 31(8), 1071-1078. https://academic.oup.com/sleep/article/31/8/1071/2454237
- Reutrakul, S., & Mokhlesi, B. (2017). Obstructive sleep apnea and diabetes: a state of the art review. Chest, 152(5), 1070-1086. https://journal.chestnet.org/article/S0012-3692(17)30865-2/fulltext
- Gottlieb, D.J., & Punjabi, N.M. (2020). Diagnosis and management of obstructive sleep apnea: a review. JAMA, 323(14), 1389-1400. https://jamanetwork.com/journals/jama/fullarticle/2764293
- Punjabi, N.M., Caffo, B.S., Goodwin, J.L., Gottlieb, D.J., Newman, A.B., O’Connor, G.T., Rapoport, D.M., Redline, S., Resnick, H.E., Robbins, J.A., Shahar, E., Unruh, M.L., & Samet, J.M. (2009). Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Medicine, 6(8), e1000132. https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000132
- Pack, A.I. (2008). Does untreated obstructive sleep apnea lead to death? Sleep, 31(8), 1067-1068. https://pmc.ncbi.nlm.nih.gov/articles/PMC2542950/
- Lim, D.C., & Pack, A.I. (2014). Obstructive sleep apnea and cognitive impairment: addressing the blood-brain barrier. Sleep Medicine Reviews, 18(1), 35-48. https://www.sciencedirect.com/science/article/abs/pii/S1087079212001360
- Kapur, V.K., Auckley, D.H., Chowdhuri, S., Kuhlmann, D.C., Mehra, R., Ramar, K., & Harrod, C.G. (2017). Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. Journal of Clinical Sleep Medicine, 13(3), 479-504. https://jcsm.aasm.org/doi/10.5664/jcsm.6506
- Rosen, I.M., Kirsch, D.B., Carden, K.A., Malhotra, R.K., Ramar, K., Aurora, R.N., Kristo, D.A., Martin, J.L., Olson, E.J., Rosen, C.L., Rowley, J.A., & Shelgikar, A.V. (2018). Clinical use of a home sleep apnea test: an updated American Academy of Sleep Medicine position statement. Journal of Clinical Sleep Medicine, 14(12), 2075-2077. https://jcsm.aasm.org/doi/10.5664/jcsm.7540
- Saletu, M.T., Kotzian, S.T., Schwarzinger, A., Haider, S., Spatt, J., & Saletu, B. (2018). Home sleep apnea testing is a feasible and accurate method to diagnose obstructive sleep apnea in stroke patients during in-hospital rehabilitation. Journal of Clinical Sleep Medicine, 14(9), 1495-1501. https://jcsm.aasm.org/doi/10.5664/jcsm.7316
- Collop, N.A., Anderson, W.M., Boehlecke, B., Claman, D., Goldberg, R., Gottlieb, D.J., Hudgel, D., Sateia, M., & Schwab, R. (2007). Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Journal of Clinical Sleep Medicine, 3(7), 737-747. https://jcsm.aasm.org/doi/10.5664/jcsm.27032
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).