Micrognathia and Obstructive Sleep Apnea: What Can be Done?

If you’ve landed here, you might be a parent who just heard the word “micrognathia” from your child’s pediatrician, or an adult with sleep apnea who’s been told your jaw position is part of the picture. Either way, I want to be upfront about something before we go any further.
I’ve lived with severe obstructive sleep apnea for more than a decade. My diagnostic AHI was 51, which put me firmly in the severe category, and I’ve been on CPAP therapy ever since. My background is in computer science, not medicine, and I write about sleep apnea because it’s the thing that quietly reshaped my life. But micrognathia isn’t part of my story. The drivers behind my OSA were different, and I’ve never used a mandibular advancement device, never had jaw surgery, and never had a clinician flag my mandible as the reason for my apnea.
So this isn’t a “here’s what I did” post. It’s a careful explainer for a condition I share an outcome with (obstructive sleep apnea) but not a cause. Where I have something useful to add from a decade of CPAP use, I’ll add it. Where I don’t, I’ll point you toward sources I trust and toward the kind of specialist who actually answers these questions for a living. This page is general information, not medical advice, and the medical disclaimer at the bottom is not a formality.
What Micrognathia Actually Is
Micrognathia, sometimes called mandibular hypoplasia, is a condition where the lower jaw is underdeveloped or significantly smaller than typical. The Cleveland Clinic describes it as a baby’s lower jaw being smaller than usual, which leaves less room for the tongue and can push it back toward the throat. That tongue position is the link between jaw size and breathing, and it’s why the condition shows up so often in sleep apnea reading.
A few things are worth getting straight at the outset.
First, micrognathia is overwhelmingly a condition diagnosed in infants and young children. The Cleveland Clinic notes that it is present at birth and is often a complication of an inherited disorder. Most cases are picked up in the first few months of life, and some are spotted prenatally on ultrasound. According to the Sleep Foundation, more than 700 different genetic mutations and inherited conditions have been associated with micrognathia, including Pierre Robin sequence, Treacher Collins syndrome, fetal alcohol syndrome, several chromosomal trisomies, and Goldenhar syndrome. It’s rarely a standalone finding.
Second, the condition can resolve as a child grows. The Sleep Foundation explains that micrognathia may go away on its own as the jaw develops, particularly through puberty. Not always, and not for every cause, but often enough that pediatric care is sometimes a matter of close monitoring rather than immediate intervention.
Third, in adults, the situation is a little different and the language gets fuzzy. Genuine adult micrognathia is uncommon and almost always reflects a childhood condition that didn’t resolve. What’s more often discussed in adult OSA settings is retrognathia, where a normally proportioned lower jaw sits further back in the face than typical. The functional consequence for the airway is similar in either case: less space at the back of the throat. But the medical picture, the diagnostic pathway, and the realistic treatment options are not identical, which is one reason why a careful evaluation matters more than a quick label.
Why a Small or Recessed Jaw Affects Breathing in Sleep
Here’s the geometry, kept simple.
Your tongue and the soft tissues at the base of it are tethered to the lower jaw. When the jaw is smaller or sits further back, those tissues end up positioned further back in the throat as well. While you’re awake and upright, your throat muscles compensate. Once you fall asleep, those muscles relax, and that already crowded space gets crowded enough to collapse partially or fully, which is the textbook picture of an obstructive apnea or hypopnea.
The numbers around micrognathia and OSA are striking. The Sleep Foundation reports that nearly 88 percent of children with micrognathia may have severe obstructive sleep apnea, compared with the much lower OSA prevalence in the general pediatric population. They also note that an average child experiences around three apneic episodes per hour during sleep, while a child with micrognathia experiences around 20. That’s roughly a sevenfold increase, and it’s a useful illustration of how much one anatomical factor can shift the picture.
For adults whose airway problems include a recessed jaw, the same physical principle applies, even if the absolute numbers depend on weight, soft tissue volume, muscle tone, sleep position, and other contributors stacked on top of the anatomy.
How Micrognathia Is Diagnosed
In infants, diagnosis is usually clinical. A small or recessed jaw is visible, and the child often has feeding difficulty, breathing pauses, or noisy breathing. According to the Sleep Foundation, around 84 percent of children with micrognathia have feeding difficulty in addition to the airway issues. From there, evaluation typically involves a craniofacial team. X-rays or CT scans are sometimes ordered to assess the jaw relative to the rest of the skull, and if breathing problems suggest sleep apnea, a polysomnogram (overnight sleep study) is the standard next step.
Adults wondering about jaw position are usually coming at it from a different direction. They’ve been diagnosed with OSA, or they suspect it, and a clinician has mentioned anatomy as part of the cause. The path here typically runs through a sleep medicine physician, sometimes with referrals to an ENT (otolaryngologist) or an oral and maxillofacial surgeon if surgical anatomy is being considered. A thorough evaluation looks at jaw position, tongue size, tonsil and adenoid tissue, palate shape, nasal airflow, and where in the airway the obstruction is actually occurring. Two adults with similar AHIs can have very different upstream causes.
Treatment: What the Options Look Like

Treatment for micrognathia depends heavily on the cause, the severity, the age of the patient, and what specifically is going wrong with breathing. There isn’t one path. There are several, and they overlap with the broader OSA treatment landscape in places.
CPAP Therapy
This is the area where I have actual lived experience to add, so I’ll spend a moment here.
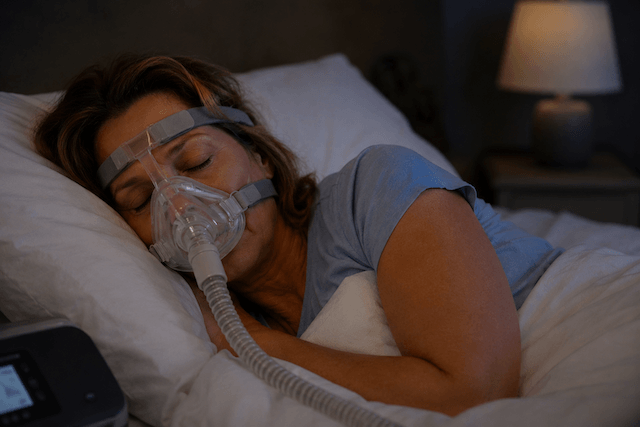
CPAP, or continuous positive airway pressure, holds the airway open by delivering pressurized air through a mask. It does not change anatomy. It compensates for it. For most people with obstructive sleep apnea, regardless of the upstream cause, CPAP is the most reliable and the most reversible therapy on offer.
The Sleep Foundation cites research showing that in adolescents and young adults with micrognathia, CPAP significantly reduced sleep apnea symptoms. They also note an important caveat: CPAP can be less effective when the airway is physically blocked by enlarged tissues rather than just narrowed and collapsible, in which case surgical evaluation may be more appropriate.
What I can tell you from my own decade of CPAP use: the therapy works, but the comfort curve is real, especially in the first few weeks. I’m a chronic mouth breather, which made a full face mask the only sensible starting point for me. If you’re a parent reading this for your child, or an adult starting therapy yourself, the early adjustment period is the part most people underestimate. I’ve written more about that in my guide to getting used to CPAP therapy, which walks through the practical side of the transition. The cardiovascular reasons to stick with the therapy, even when it’s frustrating in the early going, are also worth understanding, and I’ve covered the link between sleep apnea and cardiovascular health separately.
Mandibular Advancement Devices
A mandibular advancement device, often shortened to MAD, is a custom dental appliance worn during sleep. It looks something like a sports mouthguard but is engineered to hold the lower jaw forward by a few millimeters, opening the back of the throat and creating more room for airflow.
I have not used one. So rather than describe what it feels like, I’ll point to what the research and the major sleep bodies say about them. MADs are generally indicated for mild to moderate obstructive sleep apnea, and as an option for people who have not tolerated CPAP. Custom appliances fitted by a dentist trained in dental sleep medicine are consistently more effective and better tolerated than the generic boil and bite versions sold without a prescription. I’ve put together more on the category in my overview of sleep apnea mouth guards for readers who want a structured starting point.
For someone with a recessed lower jaw specifically, a MAD can be a logical fit because the device is doing mechanically what the anatomy has not done structurally. It’s not a fit for everyone, and it has its own tradeoffs (jaw soreness during titration and the possibility of small dental shifts over time are the most commonly cited), which is why this is a conversation to have with a dentist who actually does this work.
Pediatric Surgical Options
In infants and young children with severe micrognathia, surgical paths are sometimes necessary, especially when feeding and breathing are both compromised. Two procedures are commonly discussed.
Tongue-lip adhesion is a procedure used in infants, particularly those with Pierre Robin sequence, that brings the tongue base forward to relieve airway obstruction caused by the small jaw. It’s typically a temporary intervention used while the jaw grows.
Mandibular distraction osteogenesis (MDO) is a more involved procedure that gradually lengthens the lower jaw bone over a period of weeks using a device implanted into the mandible. The Sleep Foundation cites research showing MDO surgery resolved sleep apnea symptoms in over 80 percent of adult patients in one study, with similar results in infants. These procedures are performed by craniofacial surgeons and pediatric oral and maxillofacial specialists, not by general dentists.
Adult Surgical Options
Maxillomandibular advancement (MMA) is the most aggressive surgical option commonly discussed for adult OSA, and it’s the procedure that some adults with retrognathic anatomy eventually consider after other therapies have failed. It moves both the upper and lower jaws forward, which significantly enlarges the airway. It is a major surgery with a real recovery period, and it’s reserved for selected patients in whom the anatomy is the dominant problem and who have exhausted or rejected the alternatives. If this is on your radar, the surgeon’s specific experience with sleep apnea cases (rather than purely cosmetic or orthodontic jaw work) is the question to ask. I’ve written a broader overview of sleep apnea surgery that places MMA alongside the other surgical procedures available, for readers who want to see the wider landscape.
Positional and Lifestyle Adjustments
These don’t fix anatomy, but they can make existing therapy work better and make untreated apnea less severe in the meantime. Side sleeping rather than back sleeping reduces the gravitational pull of the tongue toward the back of the throat. Where weight is a contributing factor, weight loss can reduce the soft tissue load on an already narrow airway. Avoiding alcohol close to bedtime is widely recommended because alcohol relaxes the throat muscles in ways that make collapses more likely. None of these are substitutes for treating the underlying problem, but they’re commonly part of the conversation, and they’re worth mentioning honestly rather than pretending they’re optional extras.
Questions Worth Bringing to a Specialist
If you’re reading this on behalf of yourself or a child with confirmed or suspected micrognathia, the following questions are the kind of thing I’d want answered before agreeing to any particular treatment path:
Is the diagnosis specifically micrognathia, or is it retrognathia, or is the jaw within the normal range and the apnea coming from somewhere else? In adults especially, the distinction matters and the everyday language is loose.
How much of the obstructive apnea picture is anatomical, and how much is driven by other factors that respond to different treatments?
If CPAP is being suggested as a starting point, what should good adherence look like in the first month, and what’s the plan if it doesn’t work?
If a MAD is being considered, will it be a custom device fitted by a dentist with training in dental sleep medicine?
If surgery is being recommended, what’s the surgeon’s specific track record with sleep apnea cases, and what does the recovery actually look like?
For pediatric cases, what does the monitoring plan look like, and what are the markers that would shift the conversation toward intervention?
These aren’t questions you need to ask all at once. They’re a list to keep in your back pocket so the conversation goes somewhere useful.
A Final Honest Note
Anatomy isn’t destiny. It’s information. Knowing that the lower jaw is smaller, or set further back, tells you something useful about why your airway behaves the way it does, but it doesn’t dictate how you live with it. Some people do beautifully on CPAP. Some find a custom oral appliance changes their lives. Some, with the right anatomy and the right surgeon, get a structural fix that lasts.
What I’d resist is the temptation to pick a treatment path before the diagnostic picture is fully drawn. The reading I do, the readers who write to me, and my own experience all point in the same direction: rushing the evaluation in order to get to the treatment is how people end up on therapies that don’t quite fit them. A thorough workup with the right specialists is worth the time, even when the desire to fix the problem is urgent.
If you take one thing from this page, let it be that the OSA story you’re trying to write isn’t predestined by your jaw shape. The anatomy is one chapter. The therapy that holds your airway open through the night is the next one, and the one after that is what your sleep, your energy, and your long term health start to look like once that’s working.
I’ll see you in the rest of the site.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).