AHI Apnea-Hypopnea Index – What Your Number Actually Means
When my sleep study results came back in 2014, my AHI was 51. I had to ask what that meant. The number alone told me nothing — it was the context around it that changed everything.
The AHI, or Apnea-Hypopnea Index, is the number that defines your sleep apnea diagnosis. It’s the figure your doctor uses to determine severity, prescribe treatment, and track whether therapy is working. If you’ve just received yours, or you’re trying to understand what you’re looking at on your CPAP data, this page will walk you through everything that matters.
What the AHI Actually Measures
The AHI counts the average number of breathing disruptions per hour of sleep. It combines two types of events:
An apnea is a complete cessation of airflow lasting at least ten seconds. Your airway closes fully, breathing stops, and your brain eventually fires an emergency arousal signal to restore it — often with a gasp or snort. You may not remember these events in the morning, but your body registers every one.
A hypopnea is a partial reduction in airflow — not a complete stop but a significant narrowing of the airway that reduces oxygen delivery enough to count as a breathing event.
The formula is simple: total apnea and hypopnea events divided by total hours of sleep. If you have 51 events across one hour of sleep, your AHI is 51. That was my number. It meant I was stopping or significantly reducing breathing more than once every minute, all night, every night.
What Your AHI Score Means
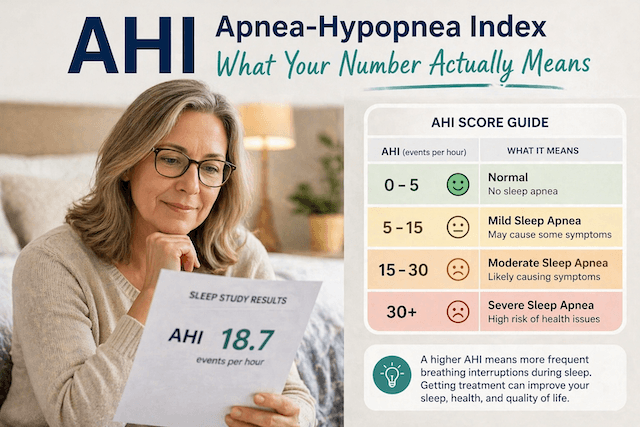
The American Academy of Sleep Medicine’s clinical guidelines define severity in four categories:
Normal: AHI under 5. Under five events per hour is considered within normal limits. Some disruption during sleep is physiologically normal; it only becomes clinically significant above this threshold.
Mild sleep apnea: AHI 5 to 15. At this level, you’re having between five and fifteen breathing events per hour. Many people with mild sleep apnea experience daytime tiredness, morning headaches, and difficulty concentrating — symptoms that are easy to attribute to other causes. Treatment options at this level include lifestyle changes, positional therapy, and oral appliances, though CPAP remains an option depending on symptom severity.
Moderate sleep apnea: AHI 15 to 30. Between fifteen and thirty events per hour. At this level, the health implications become more significant — cardiovascular stress accumulates, oxygen drops are more frequent and potentially deeper, and daytime functioning is typically more noticeably impaired. CPAP therapy is usually recommended.
Severe sleep apnea: AHI over 30. More than thirty events per hour. This is the category I was diagnosed in at 51. The cardiovascular and metabolic consequences of untreated severe sleep apnea are well-documented and serious — elevated stroke risk, hypertension, impaired glucose metabolism, and, in people like me, daily migraines from nightly oxygen deprivation. CPAP therapy is the standard first-line treatment.
One important nuance: the AHI categories don’t tell the whole story on their own. Your oxygen saturation figures — specifically how low your blood oxygen drops and for how long — provide additional clinical information that shapes treatment decisions. My blood oxygen was dropping to 78 percent, which is dangerously low regardless of the AHI number. Make sure you understand both figures when you discuss your results with your doctor.
My AHI Before and After CPAP
Before CPAP: 51. That was my baseline, measured during a sleep study that my wife insisted I get after years of watching me snore, gasp, and wake up with crushing migraines that put me in a darkened room for entire days.
First night on CPAP with the correct pressure settings: under 4. The machine kept my airway open, oxygen reached my brain properly for the first time in years, and I woke up without a headache for the first time in as long as I could remember.
Ten years later my nightly AHI sits consistently between 1 and 10. I check the myAir app every morning. Under 5 is the target and I’m usually well below it. The difference between an AHI of 51 and an AHI of 2 is the difference between the life I was living before diagnosis and the life I’ve been living since.
What a Good Treatment AHI Looks Like
Once you’re on CPAP therapy, your machine tracks your AHI nightly. The treatment goal is an AHI under 5, which indicates your therapy is effectively controlling the breathing events. Under 2 is considered excellent — your airway is being held open consistently through the night.
An AHI that stays above 5 on CPAP despite consistent use warrants investigation. Common causes include mask leak allowing the pressure to escape before it can hold the airway open, pressure settings that need adjustment, or a positional component where you’re sleeping on your back and the machine needs to work harder. Your CPAP data will show you leak rates alongside the AHI — both numbers matter for understanding whether therapy is working properly.
How AHI Is Measured
Your AHI comes from a sleep study. There are two main types.
An in-lab polysomnography is conducted in a clinical sleep centre with a full range of monitoring equipment — brainwaves, eye movements, muscle activity, breathing, oxygen levels, and heart rate all tracked simultaneously through the night. It’s the diagnostic gold standard, particularly for complex presentations or where other conditions beyond OSA are suspected.
A home sleep test uses a portable device worn for one night in your own bed. It doesn’t capture the full range of data that an in-lab study does, but for straightforward suspected OSA it’s clinically valid and significantly more accessible.

The WatchPAT One is the home sleep test I recommend — FDA-cleared, worn on the wrist, and results are reviewed by a physician. If you’re reading this page because you’ve been told you might have sleep apnea but haven’t been formally tested, this is the fastest route to a diagnosis.
What Happens After Diagnosis
Your AHI determines what treatment pathway your doctor will likely recommend.
For mild sleep apnea (AHI 5-15), options include lifestyle modifications — weight loss if indicated, avoiding alcohol before bed, sleeping on your side — as well as positional therapy for people whose AHI is significantly worse when sleeping on their back, and oral appliances that reposition the jaw to keep the airway open. CPAP is also effective at this level and may be recommended if symptoms are significant or if you prefer a more reliable solution.
For moderate to severe sleep apnea (AHI above 15, and especially above 30), CPAP therapy is the clinical standard. A machine delivers a continuous stream of pressurised air through a mask, holding the airway open so breathing events can’t occur. My AHI dropped from 51 to under 10 on the first properly calibrated night. The effect is immediate once the pressure is set correctly.

If you’ve been diagnosed and you’re at the stage of choosing a machine, my best CPAP machines guide covers what I use and what I’d recommend across different needs and budgets. Mask selection matters as much as the machine — the best CPAP masks guide covers that in detail. I’ve used the ResMed AirFit F20 full-face mask since 2014, and it’s never needed replacing with a different style.
Factors That Affect Your AHI
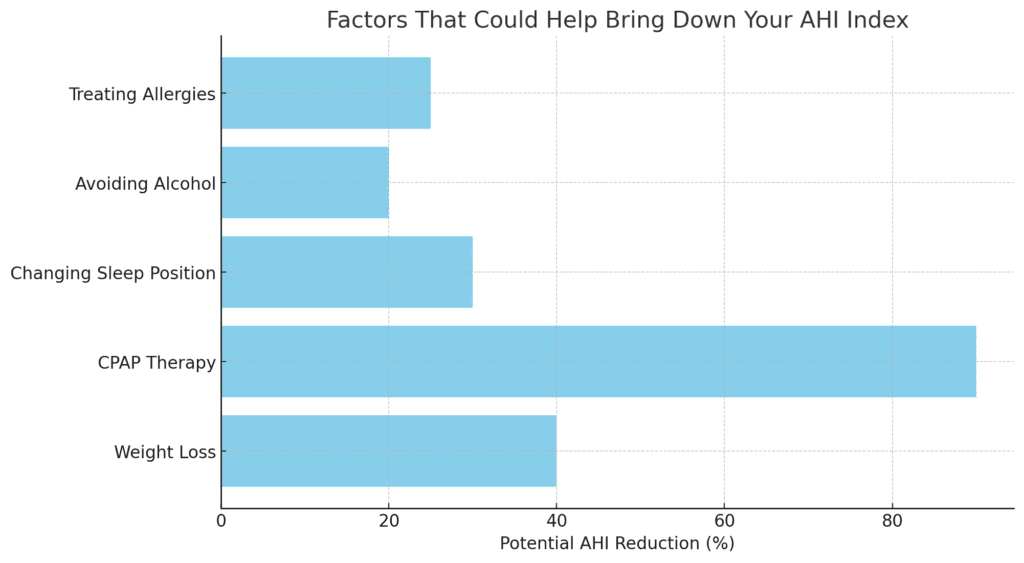
Understanding what influences your AHI helps you understand what might improve it alongside therapy.
Sleep position has a significant effect for many people. Back sleeping allows gravity to work against the airway in a way that side sleeping doesn’t, and some people’s AHI is two or three times higher on their back than on their side. This is called positional OSA and it responds well to positional therapy as either a standalone treatment or an adjunct to CPAP.
Weight is one of the most significant modifiable risk factors. Fat tissue around the neck and throat narrows the airway and increases its susceptibility to collapse during sleep. I lost weight after diagnosis, and it didn’t cure my sleep apnea — the anatomy was the primary driver in my case — but for many people, weight reduction meaningfully lowers AHI severity.
Alcohol, within a few hours of bedtime, relaxes airway musculature and reliably worsens AHI. If you’ve noticed your CPAP data looks worse after evenings when you’ve had a drink, that’s why.
Nasal congestion forces mouth breathing, which changes the airway geometry and typically worsens events. Treating chronic congestion or allergies can improve both CPAP comfort and AHI.
One Number, But Not the Only One
Your AHI is the primary metric for sleep apnea severity, but your doctor will also consider the Respiratory Disturbance Index (RDI), which includes additional subtle breathing events not captured in the AHI, your oxygen desaturation levels, and your clinical symptoms. Two people with an AHI of 20 can present very differently depending on how deeply their oxygen drops and how they function during the day.
According to research published in the Journal of Clinical Sleep Medicine, the AHI should be interpreted alongside oxygen saturation data and symptom burden rather than used as a standalone figure. The number is the starting point for the conversation, not the end of it.
What matters ultimately is what the treatment does to that number and, more importantly, what it does to how you feel. My AHI went from 51 to consistently under 10. My migraines stopped on the first properly calibrated night. My blood pressure normalised within months. The number on the app each morning is how I know the machine is doing its job.
If you’re at the start of this process and haven’t been tested yet, the most useful thing you can do is get the information. Everything follows from the diagnosis.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).