CPAP Events Per Hour: What the Number Actually Tells You

When I came home from the sleep clinic in 2014 with a diagnosis of severe obstructive sleep apnea, I was handed a CPAP machine and a rough explanation of how to use it. What I wasn’t given was any real guidance on how to read the data it produced. So I did what most newly diagnosed patients do: I stared at the numbers every morning, had no idea what I was looking at, and quietly worried.
The number that confused me most was events per hour. Mine had been 51 at diagnosis, meaning I was stopping breathing nearly once every minute across an entire night’s sleep. When the machine started reporting numbers like 2.4 or 4.8 after my first few nights on CPAP, I genuinely didn’t know whether that was good or still catastrophic. I knew it was better than 51. But better by how much? And what was I actually aiming for?
It took me a while to properly understand this number, and over a decade of checking it every morning, I’ve learned things about it that my initial sleep clinic appointment never covered. If you’re new to CPAP therapy and staring at your own readout, wondering the same things I was, this is what I wish someone had told me at the start.
If you’re completely new to sleep apnea and haven’t come across AHI yet, it’s worth reading my guide to the Apnea-Hypopnea Index first, as events per hour and AHI are essentially the same thing reported in slightly different contexts.
What Events Per Hour Actually Means
Your CPAP machine measures your breathing continuously throughout the night. Every time your airway collapses completely, cutting off airflow for ten seconds or more, that’s an apnea event. Every time it partially collapses, reducing your airflow enough to drop your blood oxygen levels, that’s a hypopnea. The machine adds these together and divides by the hours you were using it, which gives you the events per hour figure you see in the morning.
The reason this matters is that each of those events does something to your body. Your blood oxygen drops. Your brain briefly wakes you to restore breathing, usually without your awareness. Your heart works harder. Do that dozens of times an hour across a full night and the cumulative effect is what produces the exhaustion, the morning headaches, the brain fog, the blood pressure creep, and all the other consequences of untreated sleep apnea. The events per hour number is essentially a count of how often your body went through that cycle while you were asleep.
On CPAP, the goal is to prevent those events from happening in the first place. The machine delivers a continuous stream of pressurised air that acts as a physical splint for your airway, keeping it open so the collapses can’t occur. Events per hour on CPAP is your measure of how well that’s working.
The Numbers and What They Mean
The clinical scale for sleep apnea severity, set by the American Academy of Sleep Medicine, uses the same AHI thresholds whether you’re being diagnosed or tracking treated results:
| 🟢 Under 5 events per hour — Normal, treated range. This is where you want to be. 🟡 5 to 15 events per hour — Mild sleep apnea range. Therapy may be needed. 🟠 15 to 30 events per hour — Moderate sleep apnea range. See a sleep specialist. 🔴 Above 30 events per hour — Severe sleep apnea range. Requires attention. |
For context on where I started: 51 is well above the severe threshold. Getting from 51 to under 5 was the whole point of CPAP therapy, and my machine achieved it on the second night after my pressure settings were adjusted. I’ve sat between 1 and 4 most nights ever since, which is where I want to be.
The Sleep Foundation’s overview of AHI notes that CPAP therapy can reduce events per hour by around 73% in consistent users, which tracks with my experience, though my reduction was more dramatic given how high my starting point was.
Why Your Number Fluctuates Night to Night
This is the thing that confused me most in my early months on CPAP. My events per hour would be 1.8 one night and 6.2 the next, then back to 2.1 the night after. I was checking my myAir app religiously and the variation felt alarming. I kept asking myself what I’d done differently on the bad nights.
The answer, usually, is nothing. There are several things that push the number up on any given night, most of them entirely mundane.
Sleeping on your back is probably the biggest single variable. When you’re on your back, gravity pulls on your airway and makes collapses more likely. I’ve consistently noticed my events climb on nights when I’ve ended up on my back, particularly in the second half of the night when I’m more likely to roll over. Staying on your side is much better for your therapy, and if you’re finding it hard to maintain that position, a CPAP-specific pillow makes a real difference — they’re designed with cutouts that stop the mask being pushed off your face when you’re on your side, which means you’re more comfortable staying there and your seal stays intact.
Alcohol is another reliable culprit. Even one or two drinks a few hours before bed relaxes the throat muscles and makes your airway more likely to collapse during sleep. The night-after effect shows up clearly enough in the data that I can usually identify drinking nights from my myAir scores without thinking too hard about it.
Nasal congestion matters too. When I’m stuffed up with a cold or during allergy season, my events reliably go up because reduced nasal airflow affects how the machine’s pressure works. The same applies if your humidifier settings aren’t well calibrated for the season and your airway is drying out overnight.
REM sleep also plays a role. During REM your muscles are at their most relaxed, including the throat muscles that affect airway stability, so nights with more REM can show slightly higher counts as a result.
ResMed’s explainer on why AHI changes night to night covers this well from the machine’s perspective — there’s also a useful breakdown there of the role mask leaks play, which is worth reading if your numbers are jumping around without an obvious lifestyle cause.
What Actually Matters: The Trend
My sleep specialist gave me advice early on that took me a while to fully absorb: don’t look at individual nights, look at the 30-day average. She wasn’t particularly interested in a single reading of 7 or 8 if the surrounding nights were sitting at 2 or 3. What she was watching for was a sustained upward trend, or a sudden unexplained jump that held for several consecutive nights.
I’ve adopted the same approach. One night in the mild range doesn’t concern me, especially if I can identify a cause. Three or four consecutive nights above 5 with no obvious explanation is when I start paying closer attention. A gradual creep upward over a couple of weeks is when I’d get in touch with my sleep specialist.
The practical version of this looks something like: a single high reading, note it and check the next night. Two or three in a row, review your mask fit and think about whether anything has changed in your routine. A sustained elevation over two weeks or more, get it in front of someone qualified to look at the underlying data.
If your number suddenly jumps above 15 and stays there, or you’re noticing new symptoms like morning headaches, waking up choking or gasping, or worsening daytime fatigue despite using your machine consistently, don’t wait and see. You can read more about interpreting your full CPAP data to understand what else your machine is tracking alongside events per hour.
What to Do If Your Number Is Too High
I’ve had periods over the years where my events crept up and I had to work out why. The things that have reliably helped are worth going through in some detail.
Mask fit is always the first thing to check. A mask that was working well six months ago may have degraded enough that it’s now leaking air, which reduces the effective pressure at your airway and allows events to sneak through. Cushions and headgear have a finite lifespan, and it’s surprisingly easy to keep using a mask that’s quietly getting worse. If yours is more than six months old and your numbers have been drifting upward, it’s worth either replacing the cushion or trying a different mask style altogether. My guide to the best CPAP masks covers all the main options, and if you’re finding your cushion is leaking before it should, CPAP mask liners can extend the life of your seal significantly while also being more comfortable against your skin — I started using them a few years in and they made a noticeable difference to both my comfort and my leak rate.
Pressure settings are worth discussing with your sleep specialist if mask issues aren’t the explanation. The pressure your machine was set to at initial titration may not be what you need years later, particularly if your weight, anatomy, or health has changed. Don’t adjust this yourself — there’s more to it than simply turning the number up. You can read more about what pressure settings mean in my guide to CPAP pressure settings.
Sleeping position matters more than most people expect. If you’re a back sleeper, experimenting with positional adjustments can produce a meaningful reduction in events. The CPAP pillow I mentioned earlier has been one of the more effective changes I’ve made for this — keeping me comfortable on my side means I’m less likely to roll over and see my numbers spike in the back half of the night.
Something else worth considering if your events have been creeping up over time is whether your machine is giving you the data you actually need to diagnose the problem. Older machines without app support are much harder to manage — you’re flying blind compared to what the newer ResMed devices offer through myAir. If your CPAP is several years old and lacks decent data tracking, that alone can be a reason to look at upgrading. My roundup of the best CPAP machines covers the current field if you’re at that point.
If your machine is consistently showing high numbers despite everything else being in order, it’s worth considering whether CPAP is still the right therapy for you, or whether something has changed in the nature of your sleep apnea. Some people develop central or mixed apnea over time, which doesn’t respond to standard CPAP in the same way. My breakdown of CPAP versus BiPAP versus ASV explains the differences if that’s relevant to where you’ve landed.
The Number in Context
This is what a typical night looks like for me…
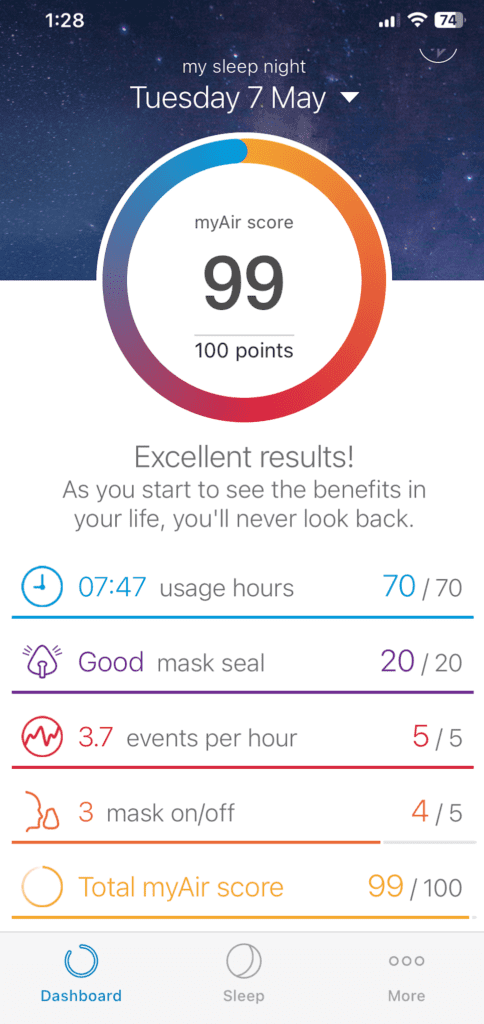
What I’ve come to understand after more than a decade of checking this number is that it’s a useful signal, not a verdict. My events per hour tells me something about how last night went, but it doesn’t tell me everything; how I feel in the morning matters. Whether my daytime energy is where I want it matters. Whether the trend over the past month looks stable or is drifting in the wrong direction matters.
On most mornings, my number is somewhere between 1 and 3. I check it on the myAir app, note it, and get on with my day. Occasionally, it’s higher, and I think briefly about why. Very occasionally, it’s above 5, and I pay more attention. Once in a while, something actually needs adjusting. That’s what ten years of consistent therapy looks like in practice: mostly unremarkable, occasionally informative, and worth the thirty seconds every morning it takes to look.
If you’ve just started CPAP therapy and you’re finding the number hard to interpret, don’t get too focused on individual readings. Get your setup right, keep the mask in good condition, stay consistent, and give the trend time to emerge. The number will tell you what you need to know.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).