How to Choose a CPAP Mask: My Experience

When my wife pushed me to get tested for sleep apnea more than a decade ago, I didn’t think much about masks. I assumed the machine was the important part. The mask was just the bit that connected my face to the air. Once I got my diagnosis and saw my AHI come back at 51, I learned how wrong that assumption was.
The mask is the part you actually live with. The machine sits on a nightstand and hums quietly. The mask is on your face for seven or eight hours a night, every night, for the rest of your life. If it leaks, you don’t sleep. If it hurts, you don’t sleep. If it makes you feel claustrophobic, you yank it off at 3 a.m. and the therapy fails.
I’m not a doctor. My background is in computer science, not medicine. What I can offer is a decade of personal experience as a chronic mouth breather on full face therapy, plus the research I’ve done while writing for this site. The goal of this guide is to walk you through the decision in plain language, with honest disclosure about what I know firsthand and what I’m reporting from the literature.
A quick disclosure before we go further. I have only ever used one type of mask, the ResMed AirFit F20. I knew from the start that I needed a full face because I sleep with my mouth open, and the F20 worked for me on the first fitting. I’ve never trialed a nasal mask or nasal pillows. The sections of this guide that cover those mask types are written in a reporter’s voice, drawn from medical research and from product specifications, not from personal experience. I think that’s the honest way to write a guide like this. You can decide whether my view is useful to you.
Why the Mask Matters More Than the Machine
The machine produces pressurized air. Every modern CPAP from the major manufacturers does that competently. They differ on auto-titration features, humidifier integration, noise levels, and data reporting, and those differences are real, but they are not the difference between therapy that works and therapy you give up on.
The mask is the difference. Peer-reviewed research published by the American Academy of Sleep Medicine notes that appropriate mask interface selection is a key determinant of treatment efficacy and compliance. Roughly two-thirds of CPAP users report mask-related side effects, including air leaks, dry mouth, skin irritation, and pressure-induced ocular issues. These side effects are the leading reason people stop wearing the device.
This is the part of the decision worth slowing down for. If you got CPAP recently and you’re already frustrated, the answer is rarely to abandon therapy. The answer is usually a different mask, a different size, or a different fitting approach. I’ve written separate guides on why your CPAP mask leaks and on CPAP dermatitis, because both of those problems have specific fixes that don’t require giving up on treatment.
The Three Main Types of CPAP Mask
There are three categories of mask in widespread clinical use. Each one solves a different problem. Choosing among them is mostly about how you breathe, how you sleep, and what feels tolerable on your face for hours at a time.
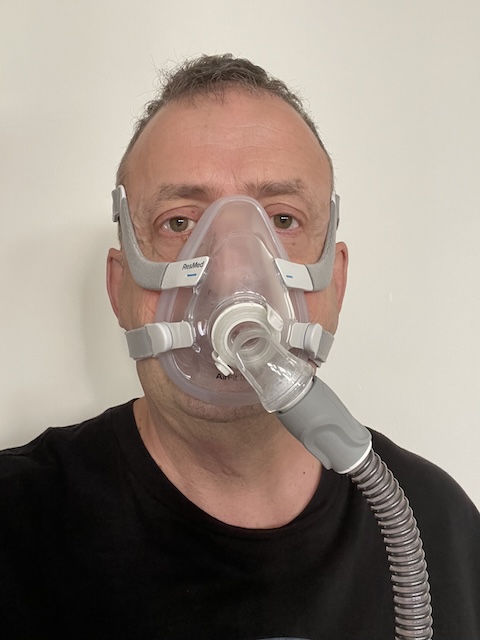
Full Face Masks

Yep, that’s me again.
A full face mask covers both your nose and your mouth. The seal runs around the perimeter of both, usually from the bridge of the nose down to just below the bottom lip. This is the mask category I wear, and it’s the one I can speak about from experience.
The case for a full face mask is straightforward. If you breathe through your mouth at night, even some of the time, a mask that only covers the nose will leak pressurized air out of your mouth and waste your therapy. A full face mask seals the whole opening, so the pressure stays where it needs to be regardless of whether you’re inhaling through your nose, your mouth, or both. They also tend to handle higher pressure settings better than smaller masks, and they’re less affected by nasal congestion when you have a cold or seasonal allergies.
The trade-off is bulk. There is more silicone touching your face. There are more contact points where leaks can develop, particularly across the bridge of the nose where small misalignments turn into air being blown straight into your eyes. Some people find them claustrophobic at first. I didn’t, but I know it’s a common reason people resist them. If anxiety is your obstacle, my piece on overcoming CPAP anxiety covers what helped me through the early months.
I’ve written a more detailed roundup of the category at Best Full Face CPAP Mask, and a comparison piece at Nasal vs Full Face CPAP Mask that goes deeper into the trade-offs.
Nasal Masks

A nasal mask covers only the nose. It sits over the bridge and seals around the base, leaving the mouth uncovered. Nasal masks are generally smaller and lighter than full face options, and they’re a popular middle ground for people who don’t need full mouth coverage but want more stability than nasal pillows offer.
The clinical case for nasal masks is interesting. Some research has actually found nasal masks to be associated with better adherence than full face masks when patients can tolerate breathing exclusively through the nose. They tend to leak less, deliver pressure efficiently, and create fewer pressure points. The catch is the word “tolerate.” If you mouth-breathe even occasionally, the therapy degrades. Some people pair a nasal mask with a chin strap to keep their mouth closed at night. Whether that works depends on the person.
I have not worn a nasal mask. What I can tell you, based on the research, is that they are most often recommended for confirmed nose breathers, for people who find full face masks too bulky, and for those at moderate pressure settings. There’s a deeper write-up on the category in my Best CPAP Nasal Masks guide.
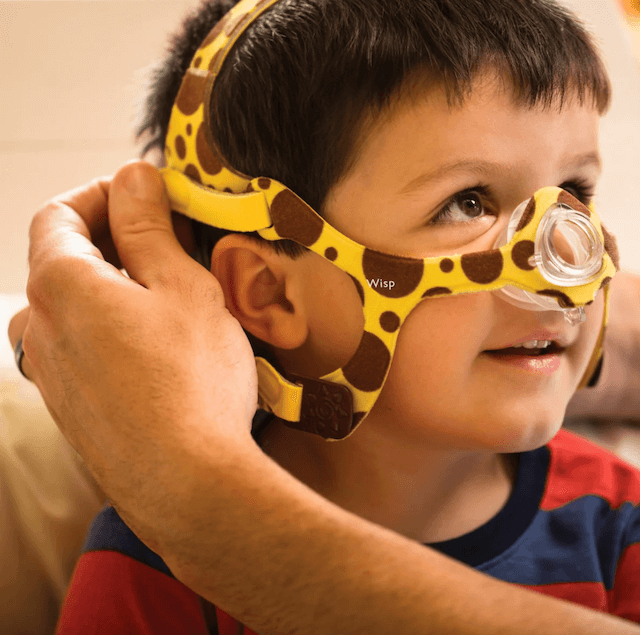
Nasal Pillow Masks

Nasal pillows are the most minimal interface available. Instead of covering the nose, two small silicone cushions seal directly at the nostril openings. The mask itself is essentially a frame and a tube. There is almost no contact with the face beyond those two seal points and the headgear that keeps everything in place.
The appeal is obvious. Nasal pillows are light, low-profile, and largely unobstructive. People who wear glasses to read in bed often prefer them because nothing crosses the bridge of the nose. People with facial hair sometimes prefer them because there’s no large surface trying to seal across a beard. Side sleepers and stomach sleepers tend to do better with nasal pillows because they don’t press against a pillow the way a larger mask does.
The limitations are also clear. Nasal pillows can be uncomfortable at high pressure settings because the air is concentrated through a small opening, which can cause a stinging sensation in the nostrils. They don’t work for mouth breathers without a chin strap. They can also dry out the nasal passages more than a mask that covers the whole nose, which is why a heated humidifier matters even more for pillow users.
For more on the differences between nasal pillows and nasal masks specifically, my piece on the difference between a nasal pillow and a nasal mask walks through them side by side. For the broader category overview, see CPAP Mask Types.
Match the Mask to How You Breathe
The single most important question to answer before you spend money on a mask is how you breathe when you’re asleep. Not how you breathe sitting at a desk. How you breathe at 3 a.m., unconscious, with your jaw relaxed.
If you breathe through your nose all night with your mouth closed, you have the widest range of options. A nasal mask or nasal pillows will probably suit you. You’ll get the lighter, less obtrusive interface, and the research suggests you may find adherence easier in this category.
If you breathe through your mouth at all, a full face mask is the safer starting point. This was my situation. I have always been a mouth breather when I sleep. My wife noticed it before I did. There was no decision to make. A nasal interface would have failed instantly because the air would have escaped through my open mouth all night, and the therapy would have done nothing. A full face solved it on day one.
If you’re not sure how you breathe, you have a few options. You can ask your bed partner to watch you for a few nights. You can record yourself sleeping with a phone. You can ask the sleep technician at your titration study, because they will have observed you. Or you can take the conservative path and start with a full face mask, which works for almost everyone regardless of breathing pattern, and switch later if you find the bulk uncomfortable. Some clinicians recommend exactly this approach for new patients.
For more on this specific question, including what to do if you’re a confirmed mouth breather, see Best CPAP Masks for Mouth Breathers.
Match the Mask to How You Sleep
Sleep position interacts with mask choice in ways that aren’t always obvious until you’ve spent a few nights with the wrong combination.
Side sleepers tend to do best with smaller, lower-profile masks. The geometry is simple. A bulky mask hits the pillow when you turn your head, and that contact pushes the seal out of position and creates leaks. Nasal pillows handle this best, followed by lower-profile nasal masks. A full face mask can work for a side sleeper, but it usually requires a CPAP-friendly pillow with cutouts that give the mask somewhere to go. I’ve covered the side sleeper question in detail at Best CPAP Masks for Side Sleepers.
Back sleepers have the easiest time. Almost any mask type works. The mask sits squarely on the face, gravity helps the seal rather than fighting it, and there’s no pillow contact to worry about. The one issue back sleepers sometimes face is air leaking upward into the eyes from the bridge of the nose, particularly with full face masks at higher pressure settings. A proper fit and the right cushion size usually solves this.
Stomach sleepers have the hardest time of any group. Almost every mask type fights the pillow when your face is turned into it. Nasal pillows are typically the best option because they have the smallest footprint. There’s a dedicated guide at Best CPAP Mask for Stomach Sleepers if this is you.
If you change positions during the night, which most of us do, the mask needs to handle all of them without resealing manually. This is where the higher end masks earn their price. Better cushion materials, more flexible frames, and more forgiving seal designs all matter when you’re tossing in your sleep.
Other Factors That Affect Mask Choice
A few situations beyond breathing and sleep position can push you toward one category over another.
Facial hair changes the math. A full beard makes it nearly impossible for a silicone cushion to seal cleanly along the cheek and jaw line, which means leaks. Nasal pillows mostly avoid this problem because they seal at the nostrils, well above the beard line. There’s a guide for this at Best CPAP Mask for Beards.
Glasses can interfere with masks that cross the bridge of the nose, particularly if you read in bed before falling asleep. Nasal pillows are the obvious workaround. Some full face masks are designed with a cushion that sits below the bridge of the nose, leaving room for glasses, and these are sometimes labeled as “minimal contact” or “under the nose” designs.
Higher pressure settings tend to favor masks with more cushion surface area. If your titration study put you on a high pressure, your sleep specialist may guide you toward a full face mask for stability, even if you’re a confirmed nose breather, because nasal pillows can become uncomfortable at high settings. There’s a separate piece at CPAP pressure settings that covers what those numbers mean.
Claustrophobia is real and common, and it usually pushes people away from full face masks toward nasal pillows. If the size of the mask is your main obstacle to therapy, the smaller the interface, the better.
Getting the Fit Right
A correctly chosen mask can still fail if it’s the wrong size or improperly adjusted. Most mask leaks are a fitting problem, not a mask quality problem.
Start with the manufacturer’s sizing template. ResMed, Philips Respironics, and Fisher and Paykel all publish printable sizing guides for their masks. Print them at actual size, hold them up to your face in front of a mirror, and compare. Most people get this part wrong on instinct because faces are not the shape we think they are.
Adjust the mask while you are lying down, not standing up. Gravity changes the geometry of soft tissue. A fit that looks perfect at the bathroom mirror often shifts the moment you put your head on a pillow.
Tighten the headgear evenly on both sides, and stop when the seal is just established. The instinct when you hear an air leak is to crank the straps tighter. This usually makes the leak worse, because over-tightening collapses the silicone cushion against your face and breaks the seal you were trying to create. The cushion is designed to inflate slightly when the machine is on, and it needs space to do that.
Use the mask fit feature on your CPAP machine if it has one. Most modern ResMed machines, including my AirSense 10, have a built-in mask fit test that runs the machine at therapy pressure for a short period and tells you whether the seal is good. It takes about a minute and removes most of the guesswork.
If your mask still leaks after a careful fit, the cushion may be the wrong size, the cushion may be worn out, or the mask may be the wrong style for your face. Cushions need replacing more often than people realize. Every one to three months is the standard recommendation, and there’s more on this in my CPAP replacement schedule post.
When to Try Something Different
Most people don’t get the mask right on the first attempt. I did, but my path wasn’t typical. If your first mask isn’t working after a fair trial of a few weeks, switching is not failure. It’s the normal way most people arrive at a mask that fits.
Reasons to consider switching include persistent leaks despite proper fitting, ongoing skin irritation that doesn’t respond to a mask liner or a different cushion material, claustrophobia that doesn’t ease with time, or air being blown into your eyes that no amount of strap adjustment fixes.
Reasons to stay the course include a mask that fits well but feels strange because you’re new to therapy, mild dry mouth that resolves once you turn up the humidifier, or general discomfort in the first few weeks that eases as your face adapts. The first month with CPAP is the hardest month. A lot of people switch masks during that period when the real issue was just adjustment, not equipment.
If you’re in that early period and struggling, my piece on getting used to CPAP therapy and the CPAP troubleshooting guide are both worth reading before you give up on the mask you have.
A Word on Cleaning and Replacement
Whichever mask you end up with, it needs cleaning. Cushions accumulate skin oil and bacteria. Headgear stretches out over time and stops holding the seal. The clear plastic frames yellow and crack. None of this is dramatic, but it adds up if you ignore it.
The basic routine is a daily wipe of the cushion with mild soap and warm water, a weekly wash of the headgear and frame, and replacement of cushions every one to three months and full masks every six to twelve months depending on your insurance coverage and the wear you’re seeing. There’s a longer breakdown in my CPAP cleaning supplies and CPAP replacement schedule guides.
Closing Thoughts
The mask is the part of CPAP therapy that decides whether you actually keep doing it. The machine matters less than people think. The mask matters more.
If I could go back and give my newly diagnosed self one piece of advice, it wouldn’t be about machines or pressure settings. It would be about taking the mask question seriously from day one. Getting the right mask is what made therapy possible for me. The fact that I happened to land on the F20 immediately is luck, not skill. Most people work through one or two before they find their fit, and that is a normal part of the process, not a sign that anything is wrong with you or with CPAP as a treatment.
If this is helpful, you might also want to read Living with Sleep Apnea for the longer story of what diagnosis and treatment have actually been like, and How to Sleep Better with Sleep Apnea for the broader picture of what has worked for me.
Be patient with the process, and don’t accept a mask that doesn’t work just because it was the first one you tried.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).