What is UPPP? A Plain Look at the Sleep Apnea Surgery
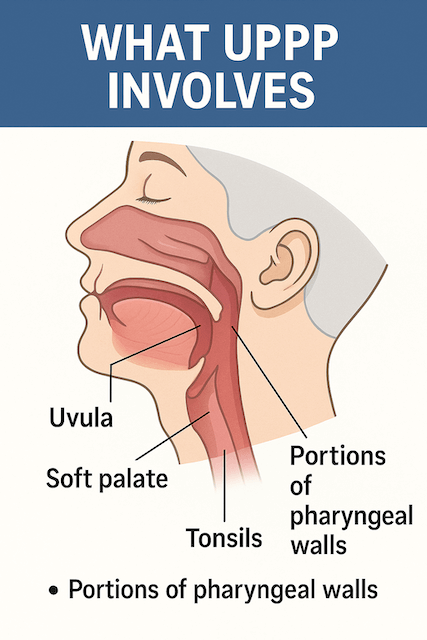
Uvulopalatopharyngoplasty, almost always shortened to UPPP, is one of the oldest surgical treatments for obstructive sleep apnea. The name covers the parts of the throat the surgeon works on: the uvula, the soft palate, and the pharynx. The goal of the operation is to widen the upper airway by removing or repositioning tissue at the back of the mouth and throat so the airway is less likely to collapse during sleep.
I have not had UPPP myself. I have used CPAP for more than a decade and no doctor has ever raised surgery as a path for me, so what follows is a research based explainer rather than a personal experience review. If you are considering UPPP, the people who matter most in your decision are your sleep physician and your ENT. What I can do here is lay out, in plain language, what the surgery actually involves, who it tends to help, how recovery generally goes, and how it compares to the other treatments most adults with sleep apnea will be offered first.
What Is Actually Removed or Reshaped
In a typical UPPP, the surgeon may take all or part of the uvula (the soft teardrop of tissue that hangs at the back of the mouth), trim or reshape part of the soft palate, and remove the tonsils if they are still there. In some cases, tissue from the side walls of the throat is also adjusted. The exact combination depends on what an examination of your airway shows and how your individual anatomy is contributing to obstruction. According to the Cleveland Clinic, UPPP may be standalone or combined with other airway procedures if more than one structural issue is contributing to apnea.
It helps to remember why this anatomy matters at all. Obstructive sleep apnea happens when the upper airway repeatedly narrows or closes during sleep, cutting off airflow until the brain rouses just enough to reopen things. The collapse can happen anywhere in the upper airway, but a large share of it involves the soft palate, which sits at the back of the roof of the mouth and acts a bit like a curtain that can fall inward when muscle tone drops at night.
A Short History of UPPP
UPPP was introduced in the early 1980s, when CPAP machines were still relatively new and surgery looked like the more practical fix for chronic snoring and OSA. For a stretch of years, UPPP was the default surgical option offered to adults with sleep apnea.
That picture has shifted. CPAP has become smaller, quieter, and far easier to live with, which has pushed surgery out of the first conversation for most people. At the same time, follow up studies have shown that UPPP results are highly dependent on the patient and that some people see their symptoms return after a few years. Newer surgical options, including hypoglossal nerve stimulation (the Inspire implant), have taken some of the demand that UPPP used to absorb.
Today, UPPP is generally reserved for people who have tried CPAP and cannot tolerate it, people whose airway examination shows clear anatomical contributors at the level of the soft palate and tonsils, and patients whose sleep apnea has not responded adequately to less invasive options. It is also sometimes considered for heavy snorers who do not meet the criteria for sleep apnea, though the Sleep Foundation notes that the trade offs of major airway surgery are hard to justify for snoring alone.
How Candidates Are Evaluated
Not every airway is well suited to UPPP, and one of the reasons modern outcomes have improved is that surgeons now use staging systems to predict who is most likely to benefit. The variables that get looked at most often are the size of your tonsils, where your soft palate sits relative to your tongue, and your body mass index. Tools like the Mallampati score try to capture some of this from a simple mouth open exam. Stage 1 candidates, whose anatomy fits the procedure most cleanly, tend to do the best. Stage 2 and 3 candidates are less likely to see lasting improvement.
The takeaway is that UPPP is not a generic fix for OSA. It is a targeted operation that does its best work when the obstruction sits at the level UPPP can actually treat. If your collapse is happening lower in the throat or at the base of the tongue, UPPP alone is unlikely to solve it, and your surgeon may discuss a multilevel approach or a different procedure entirely.
What the Procedure Involves
UPPP is performed under general anesthesia. You are asleep for the entire surgery. The surgeon props the mouth open, identifies the tissue to be removed or reshaped, and works through standard techniques to trim, reposition, or excise the relevant structures. Sutures are usually dissolvable. Depending on what is being done, the operation can take up to about two hours. Most people are discharged the same day or kept overnight so the team can confirm that breathing is stable and swallowing is safe before you go home.
Newer variants of the operation try to preserve more tissue than the original technique introduced in the early 1980s. The uvulopalatal flap, for example, folds the uvula under the soft palate instead of cutting it away entirely. Expansion sphincter pharyngoplasty and palatal advancement pharyngoplasty are other modifications designed to widen the airway with less aggressive tissue removal. The aim of these newer techniques is to keep the airway open while reducing the side effects that earlier versions of UPPP were associated with, particularly the swallowing and voice changes some patients reported.
Recovery
By most accounts, recovery from UPPP is the part patients underestimate. The throat is sore, often significantly so, for the first one to two weeks. Swallowing is uncomfortable. Talking is uncomfortable. Cold and room temperature soft foods become your friends, and anything spicy, acidic, hard, or crunchy is off the menu for a while.
The Cleveland Clinic gives a typical recovery window of two to four weeks, and notes that some people need longer depending on how extensive the surgery was. The Sleep Foundation describes a similar pattern, with two to three weeks of active recovery followed by a follow up visit to check healing and discuss next steps. One detail that often surprises people is that sleep apnea symptoms can temporarily worsen during the first part of recovery because of swelling, and using a CPAP mask comfortably right after surgery can be difficult. Your surgical team will tell you how and when to resume CPAP if you were using it before.
Most people take time off work or school during the early recovery period. Pain medication, careful oral hygiene, and rest are the main tools. If you live alone, lining up someone to drive you home and check in on you for at least the first day or two is sensible.
What the Outcomes Actually Look Like
Effectiveness is the single most discussed and most debated aspect of UPPP. It is also the part where blog posts most often overpromise.
A fair summary, drawing from the Sleep Foundation and Cleveland Clinic overviews, is this. About half of people who have UPPP see a meaningful reduction in breathing disruptions during sleep. Candidates whose anatomy fits the procedure cleanly do better than average. Snoring usually improves, at least at first, though only about half of patients keep that snoring reduction over years. UPPP rarely eliminates obstructive sleep apnea outright. Many people who have the surgery still need CPAP afterwards, though sometimes at lower pressures. Some patients see their OSA return years later as tissue heals, swells, or shifts.
The honest framing is that UPPP can move the needle for the right patient, sometimes substantially, but it is not a guaranteed cure. The Cleveland Clinic explicitly recommends discussing with your provider whether you should plan to continue CPAP after surgery as part of the treatment plan.
Risks and Side Effects
Like any surgery, UPPP carries the standard risks of bleeding, infection, and reaction to anesthesia. There are also complications more specific to this operation that are worth understanding before you say yes.
Voice changes are the one that surprises people most. Removing the uvula can change how some sounds are produced. Most patients adapt quickly and most listeners would never notice the difference, but if you speak a language that uses uvular consonants, or if your voice is your livelihood, this is a conversation to have in detail with your surgeon.
Velopharyngeal insufficiency can occur if the soft palate and throat do not coordinate properly after surgery. The clinical sign of this is liquid coming up through the nose when you drink. It is usually temporary. Nasopharyngeal stenosis, where scar tissue narrows the airway, is a less common but more serious complication that can require additional surgery to correct.
Swallowing difficulties affect a meaningful minority of patients. The Sleep Foundation notes that as many as one in three patients develop some swallowing or eating difficulty after UPPP, though most cases improve within the first few months. A small subset have persistent difficulty, particularly with thin liquids.
One practical risk that often goes unmentioned: scarring from UPPP can occasionally make CPAP harder to tolerate down the line, either because the airway behaves differently under pressure or because mask fit and seal change. That matters because, statistically, most people who have UPPP will still need CPAP at some point afterward.
How UPPP Compares to Other Treatments
It helps to see UPPP as one tool in a wider set rather than a competitor to CPAP.
CPAP remains the first line treatment for moderate and severe obstructive sleep apnea. It is highly effective when used consistently, it is not surgical, and it can be stopped or adjusted any time. Its main drawbacks are comfort, mask fit, and the discipline required to use it nightly. Most of the CPAP compliance issues people run into are solvable with better mask selection, pressure adjustments, or humidification, which is one reason surgery is usually not the first step.
Hypoglossal nerve stimulation, better known as the Inspire implant, is the newer surgical option that has taken some of the patients UPPP would have absorbed a generation ago. Instead of removing tissue, it implants a small device that stimulates the nerve controlling the tongue, gently nudging the airway open during sleep. Outcomes for the right candidates tend to be more consistent than UPPP, but Inspire is expensive, requires specific candidacy criteria, and is not appropriate for everyone.
Oral appliances, custom fitted by a dentist, gently advance the lower jaw to keep the airway open. They work best for mild and moderate OSA, are portable, and have no surgical recovery. They are not as consistently effective as CPAP for severe cases, but they are a reasonable option for people whose disease is on the lighter side or who travel constantly and want a more compact backup.
Weight management, positional therapy, and treatment of nasal obstruction can each contribute as well, and a good sleep physician will usually want to optimize the easier interventions before committing to airway surgery.
Insurance and Cost
In the United States, most insurance plans, including Medicare, will cover UPPP if it is deemed medically necessary, but the requirements are specific. There is generally a documented sleep study confirming OSA, a record of attempted and unsuccessful CPAP therapy, and a recommendation from a sleep specialist or ENT. Coverage rules vary, so the only reliable way to know what you will pay is to call your insurer with the proposed procedure codes once your surgeon has them. Out of pocket costs vary widely by region and facility.
If you are outside the United States, the rules look different in every system. Public coverage is often available where the surgery is clinically justified, but waiting times and preauthorization requirements can be involved.
Where UPPP Sits Today
UPPP is not the front line treatment for sleep apnea, and most people with OSA will never have it. CPAP and, where appropriate, oral appliances will cover the majority of cases. For people who cannot tolerate CPAP and whose airway anatomy fits the procedure, UPPP can still be a worthwhile option, and the newer, more conservative variants of the surgery have made it easier to recommend than it was a generation ago.
If you are weighing the surgery, the questions worth bringing into the consultation are practical. Where exactly is your airway collapsing, and does UPPP target that level? What stage candidate are you, and what is the expected probability of meaningful improvement? What does the surgeon expect to remove or reshape, and what are the realistic odds you will still need CPAP afterward? What does recovery look like for the specific procedures being proposed?
For my part, I have been a CPAP user for more than a decade and the therapy works for me, so airway surgery has not come up in any of my appointments. If you are in a different position, particularly if CPAP has not worked despite real effort and good support, UPPP and the alternatives mentioned here are worth a serious conversation with a sleep physician and a surgeon who specializes in sleep-disordered breathing. There is no single right answer, and the right path depends on your anatomy, your overall health, and what you have already tried.
The most important thing is not to choose between surgery and CPAP based on a blog post. Choose based on a thorough airway evaluation, an honest discussion of your options, and clear expectations about what each path can realistically deliver.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).





