Sleep Apnea Surgery: What I Have Learned

When my sleep study came back with an AHI of 51, the diagnosis was severe obstructive sleep apnea and the prescription was straightforward: CPAP therapy. But my doctor also mentioned surgery as a possibility, and the idea of being tied to a machine every night for the rest of my life made me want to understand every option before I committed.
So I spent weeks reading. I read about what each procedure actually did, how often it succeeded, who it tended to work best for, and what recovery looked like in real terms.
I want to be upfront about what this article is and isn’t. I have never had sleep apnea surgery. I never had a surgical consult with an ENT. What I had was a long conversation with my GP and my sleep doctor, and a long stretch of research. More than a decade later, I am still on CPAP and have never regretted choosing it. But the work I put in while making that decision shaped how I think about treatment options, and it is worth sharing for anyone trying to make the same call.
One personal detail does matter here. Years before my sleep apnea diagnosis I had a septoplasty to straighten a deviated septum, which was done for general breathing issues rather than for sleep apnea. The surgery helped my daytime breathing, but it did not prevent the obstructive sleep apnea that showed up later. That experience taught me something important: a nasal procedure can help with airflow without necessarily addressing where your real obstruction is occurring.
What sleep apnea surgery actually is
Sleep apnea surgery is not a single procedure. It is a family of procedures that try to change the physical structure of your airway so it does not collapse when you sleep. Some target the nose. Some target the soft palate or tonsils. Some target the tongue base. Some go after the jaw itself. One option, technically a surgery, implants a small device that nudges your tongue forward at night.
Surgery is almost never the first treatment a doctor reaches for. Continuous positive airway pressure remains the most effective and least invasive option for most people with moderate to severe OSA. The American Academy of Sleep Medicine guideline on surgical referral puts surgery in context. It is for people who cannot tolerate CPAP, who have failed to adhere to it despite genuine effort, or who have an obvious anatomical issue surgery could correct. PAP comes first.
The other thing worth understanding upfront is that surgery is not one size fits all. Your anatomy decides what might work for you. Two people with the same AHI can have completely different obstruction patterns, and the same procedure can be a brilliant fix for one and useless for the other.
The procedures I read about
Uvulopalatopharyngoplasty (UPPP)
UPPP is the most common surgery performed for sleep apnea in the United States. The surgeon removes or reshapes tissue in the throat, usually including parts of the uvula, the soft palate, the tonsils, and the back of the throat. The goal is to widen the airway behind the mouth.
What I found in the research was that UPPP has a mixed reputation. Reported success rates vary widely depending on how you define success. A 50 percent reduction in AHI is a very different bar than getting AHI below 5. Younger patients with smaller body mass, less severe sleep apnea, and clear soft palate obstruction tend to do best. Patients with my profile, severe OSA, did not show the same outcomes on average.
The complications that gave me the most pause were swallowing changes, voice changes, and the possibility of nasal regurgitation. Some patients also reported that initial improvements faded over time as tissues changed with age and weight.
Maxillomandibular advancement (MMA)
MMA is the most aggressive of the common procedures. The surgeon breaks both the upper and lower jaw and moves them forward. The result is a dramatically wider airway from front to back. Recovery is measured in months, not weeks.
The research consistently put MMA at the top of the success rate tables for severe OSA. If a single procedure was going to work for someone with an AHI like mine, this was the one most likely to do it. But the trade offs were significant: hospitalization, weeks of difficulty eating, the possibility of lasting facial numbness, and a real change in facial appearance, since the jaw is being repositioned by several millimeters.
For people who have exhausted other options and cannot tolerate CPAP, MMA can be a serious answer. For me, choosing it as a first move with a treatment as effective as CPAP already available felt out of proportion to the problem.
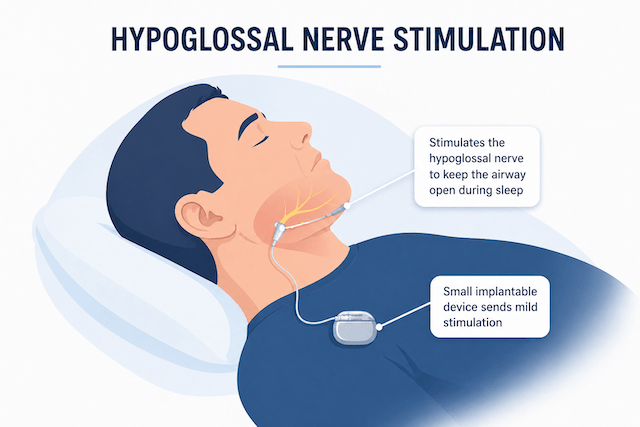
Hypoglossal nerve stimulation (Inspire)
Hypoglossal nerve stimulation, most commonly known by the brand name Inspire, is the newest of the options I looked at. It is technically a surgery, but the procedure itself is far less invasive than UPPP or MMA. A small device is implanted under the skin in the chest, with a lead that runs to the hypoglossal nerve, the nerve that controls tongue movement. When you breathe in at night, the device delivers a gentle stimulation that pushes the tongue slightly forward, keeping the airway open.
The appeal is real. The procedure is outpatient or near outpatient for most patients. The device is adjustable. It can be turned off or removed. And the published results are encouraging for the right candidates.
The catch is that the right candidate window is narrow. Eligibility typically requires a BMI under a certain threshold, an AHI in a defined range, and the absence of certain airway collapse patterns that can only be confirmed with drug induced sleep endoscopy. There is also the matter of cost, the eventual need for battery replacement surgery, and limits on the kinds of MRI scans you can have afterward.
Genioglossus advancement
This procedure pulls the tongue muscle forward by cutting a small piece of the chin bone with the tongue attachment still on it and repositioning it. It is rarely done by itself anymore. Most surgeons use it as part of a multilevel approach, paired with UPPP or other throat work.
Nasal surgery
I paid close attention to this category because of my own history. Septoplasty, turbinate reduction, and treatment of nasal polyps are all procedures aimed at the nose itself, not at the throat or tongue.
Here is the important caveat the Mayo Clinic makes plain: nasal surgery is generally not a direct treatment for OSA. It can improve nasal breathing, which can in turn make CPAP much easier to tolerate at lower pressure, and it can sometimes reduce mouth breathing. But if your primary obstruction is at the throat or tongue base, fixing your nose will not fix your sleep apnea.
That mirrored my own experience. My septoplasty helped me breathe through my nose during the day, but I went on to develop severe OSA anyway, because the real obstruction in my case was happening further back. If you are considering nasal surgery hoping it will resolve your sleep apnea, talk to your doctor about where your obstruction is actually occurring before signing up for any procedure. For people with a known deviated septum and CPAP intolerance, the order can matter: nasal work first to make CPAP tolerable, rather than nasal work as a cure on its own.
Soft palate implants
The Pillar procedure involves placing small implants in the soft palate to stiffen it and reduce vibration and collapse. It is the least invasive option I looked at, but it is also the least powerful. The research generally limits it to mild OSA. With an AHI of 51, this was never going to be enough for me.
Tongue base procedures
Lingual tonsillectomy, tongue base reduction, and similar procedures aim at reducing or repositioning tongue tissue. Like genioglossus advancement, these are usually performed as part of a multilevel surgical plan rather than as a standalone fix. The complication that always made me hesitate when reading about tongue base procedures was speech and swallowing risk. The tongue does a lot of work every day, and any procedure that touches it deserves careful consideration.
The modern multilevel approach
One pattern I noticed in newer research was that fewer surgeons treat sleep apnea as a single procedure problem anymore. The modern approach is multilevel, meaning the surgeon identifies every site where obstruction is happening and addresses each one, sometimes in a single surgery and sometimes staged across more than one operation.
This is where drug induced sleep endoscopy, called DISE, comes in. A patient is brought to a light sleep with medication, and the surgeon uses a small scope to watch where the airway actually collapses. That information drives the surgical plan. Without DISE or comparable imaging, choosing a procedure feels closer to guesswork than I was ever comfortable with.
For anyone seriously considering surgery, asking about DISE or another method of obstruction mapping is reasonable. Surgery aimed at the wrong level of your airway is unlikely to help, and it is not something you can easily undo.
Why I chose CPAP
I did not have a surgical consult. I read, I thought about it, I talked with my GP and sleep doctor, and I made a decision. Several things pushed me toward CPAP rather than surgery.
The first was certainty. CPAP, when you use it correctly, works for almost everyone with OSA. Surgical success rates, even for the most effective procedures, do not reach that level. For someone with severe sleep apnea, the gap was meaningful.
The second was reversibility. If CPAP did not work for me, I could try a different mask, a different machine, or a different therapy entirely. Surgical changes are permanent. If a procedure did not produce the result I wanted, I would still need CPAP, but I would also be living with whatever the surgery had changed in my throat or jaw.
The third was the risk profile. The downsides of CPAP therapy are mostly inconveniences: mask leaks, dry mouth, the occasional bout of aerophagia, the learning curve of getting used to sleeping with something on your face. They are real but manageable. The risks of surgery, even routine surgery, are different in kind: anesthesia, infection, the possibility of permanent changes to swallowing or breathing, and the possibility that the procedure simply does not work and you still need CPAP afterward.
The fourth was time. I could start CPAP within weeks. Surgery would have meant evaluation, scheduling, recovery, and a period of uncertainty about whether it had worked. CPAP gave me an answer almost immediately.
The fifth, and perhaps the most underrated, is that CPAP is something I control. I can change my mask. I can adjust my pressure settings with my doctor. I can travel with it. I can review my data every morning if I want to. Surgery is a single event with permanent consequences. CPAP is an ongoing therapy I can tune as my needs change.
More than a decade in, my AHI on CPAP is well controlled, my sleep is far better than it was before diagnosis, and I have never had to revisit the surgery question. I am not anti surgery, and I will not tell you to make the same choice I made. The math worked out the way it worked out, and I am glad it did.
Who should actually consider surgery
Despite my own choice, there are people for whom surgery is the right call. Reading the AASM guideline and the more recent literature, the candidates who seem to benefit most have some combination of these traits: a documented inability to tolerate CPAP despite genuine effort with different masks and pressure settings, a clearly identifiable anatomical obstruction that a specific procedure can correct, a BMI in the favorable range for the procedure being considered, younger age, and realistic expectations about outcomes.
For people who meet those criteria, hypoglossal nerve stimulation has become a genuinely promising option in the last decade. MMA remains the most effective surgical treatment for severe OSA when it is appropriate. UPPP still has a role for the right anatomy, particularly when combined with other procedures.
The wrong reasons to pursue surgery are also worth naming. Wanting to avoid a CPAP machine without giving CPAP a serious trial is a poor reason. Wanting a fast fix is a poor reason. Believing that surgery is guaranteed to work is a poor reason. Going in with realistic expectations, supported by appropriate workup and a surgeon who can answer hard questions about their personal success rates rather than general literature averages, is the better starting point.
Things worth trying before surgery
If you have been told to consider surgery because CPAP is not working for you, it is worth checking whether CPAP is really not working or whether CPAP has not been properly optimized for you. Many people who have struggled with the therapy have not yet tried the variables that often make the difference.
The mask is the biggest one. Mask type matters enormously. Nasal pillows, nasal masks, and full face masks suit different anatomies and breathing patterns. As a chronic mouth breather, I needed a full face mask from day one. A nasal mask would have failed me, and if I had judged CPAP on that basis I would have given up on it. Worth confirming you have the right mask before concluding the therapy has failed.
Pressure settings are the next variable. Static CPAP and auto-adjusting CPAP behave differently, and the wrong pressure can make therapy uncomfortable and ineffective at the same time. A sleep doctor or CPAP technician can review your data and adjust.
Humidification is often the difference between feeling rested and waking up with a dry throat. Chin straps help some mouth breathers who are using nasal masks. Anxiety about CPAP, particularly in the early weeks, is more common than people admit and is treatable with gradual exposure and patience.
Beyond CPAP itself, there are non surgical alternatives worth investigating. Oral appliances advance the lower jaw and can work for mild to moderate cases. Positional therapy helps people whose apnea is significantly worse on their back. Weight loss, when applicable, can meaningfully reduce severity. Treating nasal congestion, avoiding alcohol close to bed, and looking at the broader landscape of alternative treatments can all matter.
If you have worked through all of that and CPAP is still not viable, then a surgical conversation is the right next step. But the order matters.
Final thoughts
Sleep apnea surgery is not wrong. It is a real option that has helped real people. For the right anatomy, the right severity, and the right candidate, procedures like Inspire or MMA can be genuinely life changing.
What I learned during my own decision making is that the success of any surgery depends on a long list of variables, most of them outside your direct control, and that the certainty offered by CPAP is hard to match. With severe OSA and the kind of risk tolerance I have, CPAP gave me the highest chance of treating the underlying problem with the least permanent risk. That math has held up.
If you are weighing this decision, do the reading. Talk to a sleep specialist about where your obstruction is happening. Ask a sleep surgeon hard questions, not just about general literature but about their specific outcomes with patients like you. Get more than one opinion. And do not let anyone, including yourself, push you toward a decision faster than you are comfortable making it.
The goal is not to avoid CPAP or to avoid surgery. The goal is to treat sleep apnea effectively so that the years ahead are healthier and more energetic than the years before diagnosis. There is more than one road to that outcome.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).