Positional Therapy for Sleep Apnea: Does it Work?
“This post contains affiliate links. I may earn a commission if you buy through these links at no extra cost to you. Read my Disclaimer for more details.”

When I was diagnosed with obstructive sleep apnea in 2014, my AHI was 51 and my blood oxygen was dropping rapidly at night. My doctor’s exact words were that CPAP wasn’t optional — it was life-saving. There was no conversation about alternatives, no discussion of sleeping position, no suggestion that anything short of a machine forcing air into my airway at pressure was going to cut it. For me, that was correct. My breathing events were happening across all sleep positions and with a severity that positional changes alone would never have touched.
But I’ve since spoken to a lot of people in the sleep apnea community whose situations are genuinely different from mine, and one of the things that comes up regularly is positional therapy — the idea that for some people, the position they sleep in is the dominant factor in their apnea, and that addressing it directly can be a legitimate treatment rather than just a lifestyle tweak.
The question I want to answer here is a simple one: Does positional therapy actually work? Who is it actually for, and what are your practical options if you want to try it? I’m going to be honest about the limits of what it can achieve, because I think some of the marketing around positional devices overpromises significantly. But I also think it’s genuinely underused for the specific subset of people it suits.
Why Sleeping Position Affects Sleep Apnea
The mechanics are fairly straightforward once you understand what’s happening in the airway during an apnea. When you lie on your back, gravity pulls the tongue and soft palate backward toward the throat. For someone with a naturally narrower airway — due to anatomy, excess tissue, or reduced muscle tone — that posterior displacement is often enough to cause partial or complete obstruction. Roll onto your side, and gravity is no longer working against you in the same way. The airway sits differently, the tongue falls forward rather than back, and the obstruction either doesn’t occur or occurs much less frequently.
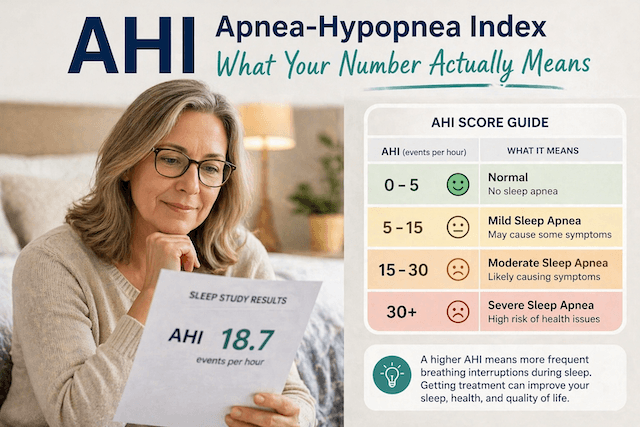
The American Academy of Sleep Medicine recognises positional obstructive sleep apnea as a distinct clinical entity, defined as having at least twice as many apneas in the supine position as in non-supine positions. Research suggests that somewhere between 30 and 50 percent of people with OSA meet this definition — meaning their breathing problems are significantly driven by back-sleeping rather than being equally bad in all positions. For those people, positional therapy isn’t a workaround. It’s treating the actual problem.
For the other half of the OSA population — people like me — the apnea is happening regardless of position, and the severity is such that sleeping on your side would help somewhat, but never enough. That distinction matters enormously, and it’s the reason the first thing anyone considering positional therapy should do is look at their sleep study data.
The Number You Need to Know
If you have a sleep study report, find the breakdown of your AHI by position — usually listed as supine AHI and non-supine or lateral AHI. If your supine AHI is more than twice your lateral AHI, you have positional OSA, and you’re a reasonable candidate for positional therapy. If the two numbers are similar, positional therapy is unlikely to make a meaningful difference, and you need to focus on other treatment options.
As a rough guide, a supine AHI of 24 and a lateral AHI of 4 represents the kind of positional difference where addressing sleep position could genuinely normalise your breathing. A supine AHI of 32 and a lateral AHI of 28 represents a non-positional pattern where the position is barely a factor.
If your sleep study didn’t record positional data, or you only did a home test that didn’t track it, it’s worth asking your doctor whether a fuller study would be appropriate before investing in positional devices. The Sleep Foundation’s overview of positional sleep apnea is a good plain-language resource if you want to understand the clinical framework before that conversation.
Does the Evidence Actually Support It?
Yes, for the right candidates. A 2021 meta-analysis published in Sleep Medicine Reviews, which looked at over 1,500 patients with confirmed positional OSA, found that positional therapy reduced AHI by an average of around 54 percent and achieved treatment success — defined as AHI below 5 — in roughly a third to half of patients, depending on baseline severity. Adherence rates at six months were comparable to or better than CPAP adherence rates for mild OSA.
The honest interpretation of those numbers is that positional therapy works well for people with mild to moderate positional OSA, works less reliably as severity increases, and doesn’t work at all if the apnea isn’t primarily positional. It also works as a supplement to other treatments — combining it with an oral appliance, for example, or using it alongside CPAP to reduce required pressure. It’s not a miracle solution but it’s also not a gimmick.
Before You Buy Anything: The DIY Test
If you haven’t confirmed whether your OSA is positional yet and you want a low-cost way to test the concept before spending money on a device, try a few nights with a rolled towel or a small backpack worn on your back to prevent you rolling supine. It’s not comfortable, and you won’t want to do it long-term, but it will tell you fairly quickly whether staying off your back is making a noticeable difference. If you wake up feeling better, snoring less, and your CPAP data (if you use one) shows fewer events, that’s a meaningful signal worth acting on.
The Two Products I Recommend
For people who’ve confirmed their OSA is positional and want a proper solution, these are the two options I point people toward. Both are a similar price point.
MedCline Acid Reflux Relief Wedge + Body Pillow System

The MedCline system creates a supported sleeping environment that makes side-sleeping comfortable and back-sleeping mechanically difficult. The wedge elevates your upper body at a 15 to 20-degree incline, while the full-length body pillow keeps you laterally positioned through the night.
It was originally developed for acid reflux and GERD. If you’re someone whose sleep apnea coexists with reflux, which is more common than people realise, the two conditions share several risk factors — this is the product that addresses both problems simultaneously rather than requiring separate solutions. It takes up significant bed space and isn’t portable, so it’s a different kind of commitment to the Rematee. But for people who want maximum comfort and have the room for it, the MedCline system is the most complete positional solution available.
Price $269.99 Available from Sleep Doctor.
MedCline Shoulder Relief System

One of the less-discussed barriers to positional therapy is that side-sleeping is genuinely uncomfortable for a significant number of people — particularly those with shoulder pain, rotator cuff issues, or joint problems that make lying on their side painful enough to wake them. If that’s what’s been keeping you sleeping on your back in the first place, a standard positional belt isn’t going to solve the problem because discomfort will just win.
The MedCline Shoulder Relief System is specifically designed for this situation. It uses a built-in arm pocket that eliminates direct downward pressure on the shoulder, combined with the same incline and body pillow support as the reflux system. The result is a neutral arm position that most people with shoulder pain find dramatically more comfortable than conventional side-sleeping. It creates a 10-degree incline rather than the steeper 15 to 20 degrees of the reflux system, so it’s a slightly more gentle elevation overall.
If chronic shoulder pain has been the reason you default to sleeping on your back, this is the product to look at. It solves two problems at once rather than expecting you to choose between your shoulder and your airway.
Price $269.99 Available from Sleep Doctor.
Choosing Between the Two
The decision between the MedCline systems comes down to one question: is shoulder pain part of your picture?
If you have positional OSA with no significant shoulder issues, the Reflux Relief system is the right choice — particularly if you also deal with reflux or GERD, where the 15 to 20 degree incline addresses both problems at once. If shoulder pain has been the real reason you keep defaulting to sleeping on your back, the Shoulder Relief system solves that problem first and the positional OSA second. There’s no point investing in a side-sleeping solution if side-sleeping itself is too painful to sustain.
Both systems are a serious commitment in terms of bed space and cost, which is worth being honest about. If you want to test whether positional therapy is right for you before spending at this level, the DIY backpack or rolled towel method described earlier is a reasonable proof of concept first. But if you’ve already confirmed your OSA is positional and you want a long-term solution built for comfort, the MedCline range is the best available.
What to Be Realistic About
Positional therapy won’t work if your apnea isn’t primarily positional. It won’t work if you have severe OSA, and events are happening at a high rate regardless of position. For those people — and I include myself in that group — CPAP is the treatment, and no amount of sleeping on your side changes that fundamental picture.
But I think the sleep medicine world has historically been too quick to default to CPAP for everyone, including people with mild positional OSA for whom something much simpler might be entirely adequate. If you’re someone who has tried CPAP and genuinely cannot tolerate it, or if you have mild positional OSA and want to explore what’s appropriate before committing to a machine long-term, positional therapy deserves a proper trial rather than being dismissed as insufficient without testing it against your actual numbers.
If you’re using CPAP and your OSA isn’t mild, positional therapy can still earn its place as a supplement. Staying off your back tends to reduce the pressure your machine needs to deliver, which improves comfort and often improves adherence. It’s not an either/or choice.
The honest path is to look at your sleep study data, understand whether your OSA is positional, use the DIY method to test the concept at no cost, and then invest in one of the MedCline systems if your own body’s evidence supports it. That’s not a complicated process — but it does require getting the data rather than guessing.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).