Mouth Breathing, Sleep Apnea, and Low Testosterone: My Story

Some things are harder to write about than others. The fatigue, the brain fog, the snoring – those are easy. Nobody feels embarrassed talking about being tired. But when living with sleep apnea started affecting other parts of my life, the parts that feel more private, it took me a long time to even admit it to myself, let alone do anything about it.
I’ll get to that. But first, some context.
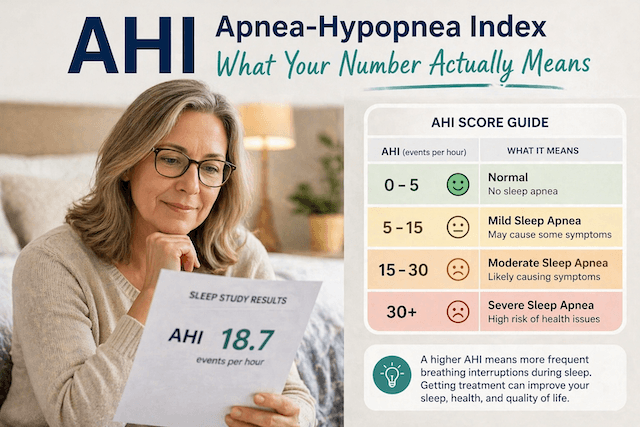
When I was diagnosed with severe obstructive sleep apnea, the doctor’s focus was on keeping me alive, essentially: getting me onto CPAP therapy, getting my oxygen levels stable, and addressing the migraines I’d been having. I started with a full-face mask; my numbers improved dramatically, and within a few days, I felt genuinely transformed—more energy. Clearer head. The relief was enormous.
But about six months in, something felt off. My CPAP compliance was solid and by every measurable standard my sleep apnea was being managed. Yet I still felt flat in a way I couldn’t quite explain. Tired in a different way than before. Struggling to maintain muscle despite exercising regularly. And yes, a noticeable drop in libido. That’s the part that was hardest to sit with, because it felt like something fundamental was slipping away from me without any obvious explanation.
I eventually got blood work done. My testosterone was sitting in the low-normal range for my age. Not dramatically low, but low enough to explain a lot of what I’d been feeling.
The Breathing Connection I Hadn’t Considered
What followed was a lot of reading, a lot of conversations with my doctor, and gradually a clearer picture of what was happening. The short version is that how you breathe while you sleep matters far more than I’d ever realised, and I’d been getting it wrong even with the CPAP on.
I was mouth breathing. I still use a full face mask, which covers both the nose and mouth, and while that solves the mechanical problem of the airway collapsing, it doesn’t stop you from defaulting to mouth breathing throughout the night. And that turns out not to be the same thing as breathing properly.
When you breathe through your nose, your nasal passages produce nitric oxide, which dilates blood vessels and improves how efficiently oxygen is delivered through your body. Mouth breathing bypasses all of that. Your nose also filters and warms the air, maintains a better carbon dioxide balance, and keeps the body in a more settled physiological state. Mouth breathing, especially during sleep, can keep your system in a kind of low-level stress response. And chronic stress, the hormonal kind, suppresses testosterone. The two are essentially in competition: when cortisol is high, testosterone tends to be low. Your body prioritises survival over everything else.
I’m not going to pretend I fully understood all of this at the time. What I did understand was that even though my sleep apnea was being treated, I wasn’t breathing optimally, and that gap seemed to matter.
What the Research Actually Shows About CPAP and Testosterone
Here’s the thing I wish someone had told me earlier, because it would have saved me several months of waiting for a result that wasn’t coming: CPAP therapy doesn’t reliably increase testosterone levels. I assumed that fixing my sleep would fix my hormones. The evidence says otherwise. Multiple studies have looked at this, and the consistent finding is that CPAP treatment does not produce significant changes in testosterone, even in men whose levels were low to begin with.
That was genuinely frustrating to discover. But it also made sense once I understood that testosterone is affected by a lot of overlapping things: sleep quality, body composition, stress, age, and yes, breathing patterns. A 2019 meta-analysis covering hundreds of OSA patients found no significant testosterone improvement after CPAP treatment. Treating one piece of the puzzle doesn’t automatically restore balance across all the others.
What CPAP does improve is sexual function more broadly. The research on erectile dysfunction and sleep apnea is more encouraging: most men with OSA who start CPAP report improvement there. But the underlying testosterone picture was a separate problem that needed separate attention.
Working On the Mouth Breathing Problem
Because I still use a full face mask, I couldn’t simply switch to a nasal-only setup and call it solved. What I could do was pay more attention to whether I was actually using my nose, and try to encourage it. I worked on clearing my nasal passages more consistently, which for me meant addressing some chronic congestion that had quietly been nudging me towards mouth breathing every night. My deviated septum wasn’t helping with that either, which I’ve written about separately. Saline rinses, sorting out allergies, and using a CPAP humidifier properly so the air wasn’t so dry made a meaningful difference. The dry mouth I’d been waking up with most mornings improved noticeably.
It’s not a perfect solution, and I won’t pretend it produced a dramatic hormonal turnaround. But reducing the degree of mouth breathing, even while keeping the same mask, seemed to help in ways I could feel if not always measure: better energy through the day, less of that groggy-despite-sleeping feeling, and generally feeling more like myself.
The Weight Issue
I have to be honest about this part, even though it’s uncomfortable in a different way. The research on sleep apnea and testosterone points quite clearly to body weight as a significant, possibly primary, driver of the hormonal picture. Excess weight, particularly around the neck and abdomen, affects the airway and suppresses testosterone through several mechanisms. The link between carrying extra weight and sleep apnea is well established, and the hormonal connection runs alongside it.
Over about 18 months, I lost roughly 25 pounds. I did this through a combination of strength training three or four times a week and eating better, mostly cutting out the processed stuff and making sure I was eating enough protein. Nothing extreme, nothing that didn’t stick. The difference in my testosterone levels was more noticeable than anything else I tried. It moved from low-normal into the middle of the normal range, and that shift, while it doesn’t sound dramatic on paper, felt significant in everyday life.
The other thing I noticed is that the relationship between CPAP therapy and weight runs in both directions. When I was sleeping badly, I was too exhausted and too foggy to exercise properly or make good food choices consistently. Getting the sleep right first made the weight management more achievable. The two things fed each other in a good way once I had them both moving in the right direction.
The Testosterone Replacement Question
At some point in this process, I started looking into TRT, which felt like the obvious question: if my testosterone was low, why not just replace it? The answer is more complicated than I expected, and it’s worth knowing about if you’re in a similar position.
Testosterone replacement can worsen sleep apnea. There’s reasonably consistent evidence for this: TRT affects how the body responds to oxygen drops during sleep, and research has found that men starting TRT can see their breathing disruptions during sleep increase significantly. Untreated or poorly controlled OSA is generally considered a reason not to start TRT. And even for men with well-controlled sleep apnea on CPAP, monitoring needs to be close if TRT is introduced.
That catch-22, sleep apnea suppresses testosterone, but treating the testosterone can make sleep apnea worse, is genuinely frustrating. I decided against TRT. My levels weren’t clinically in the hypogonadal range, and the risk of undermining the sleep apnea control I’d worked so hard for didn’t seem worth it. I focused instead on everything I could influence: breathing, weight, sleep quality, and stress. If my levels had been more severely low, I’d have had a different conversation with my doctor, but it would have needed to happen alongside excellent CPAP compliance and careful monitoring.
On Stress, and Why It Matters More Than You’d Think
I’m not someone who goes in for a lot of wellness language, so I’ll try to say this plainly. Chronic stress suppresses testosterone. Full stop. And living with untreated or poorly managed sleep apnea is physically stressful in ways you can’t feel because they’re happening while you’re asleep. Every time your airway collapses and your oxygen drops, your body responds as if there’s a threat. That stress hormone response, repeated dozens or hundreds of times a night for years, leaves a mark.
Once my sleep was genuinely stable, my resting state felt different. Less reactive. Less wired. I started sleeping and waking at consistent times, cut caffeine off earlier in the afternoon, and made sure my CPAP setup was dialled in properly so I wasn’t waking up uncomfortable in the night. None of that is revolutionary advice, but the cumulative effect of getting all of it right at the same time was more than the sum of the parts.
What I’d Say to Someone in the Same Position
If you’ve been on CPAP for a while and things still feel off, it’s worth asking whether you might be mouth breathing through the night. It’s not something your machine will flag as a problem if the basic therapy numbers look good. Check your CPAP data for leak rates, and pay attention to whether you’re waking up with a dry mouth or sore throat. Those are signs worth taking seriously.
If you’re noticing fatigue, difficulty building or maintaining muscle, a decline in libido, or just a persistent flatness that doesn’t match how well you think you’re sleeping, get blood work. Get your testosterone checked in the morning, when levels are at their peak. Don’t guess.
And if the results show you’re low, understand that the path back isn’t usually a single fix. For me, it was a combination of addressing the mouth breathing as best I could, losing weight, exercising consistently, and giving my body time to recalibrate. None of that happened quickly. But it did happen.
The topic feels personal because it is. But it’s also more common among men with sleep apnea than most people know, and the fact that it doesn’t get talked about openly doesn’t mean you’re dealing with it alone.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).