Central Sleep Apnea: Causes, Symptoms, and Solutions
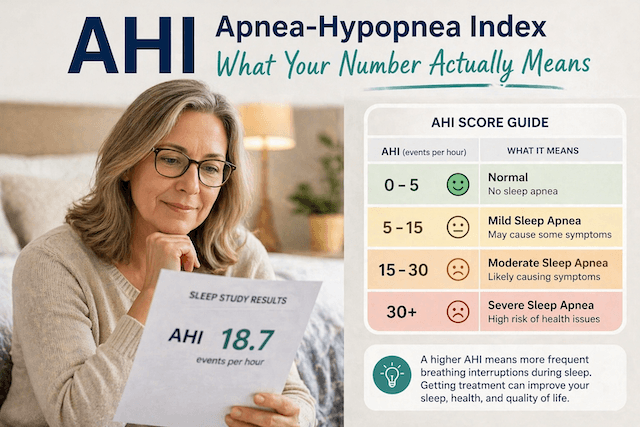
When I was diagnosed with obstructive sleep apnea in 2014, I thought I understood what sleep apnea was. The airway collapses, you stop breathing, CPAP props it back open, problem solved. That model held up fine for my own situation. My AHI was 51, my treatment is CPAP, and after over a decade of using my ResMed AirSense 10 every night my therapy data is consistently good.
But over the years, as I’ve read more widely about sleep medicine and heard from readers and fellow CPAP users, I kept encountering a different kind of sleep apnea that didn’t fit that model at all. One where the airway isn’t the problem. One where CPAP doesn’t always fix things the way you’d expect. One that’s quieter and in some ways more confusing than the condition I have.
Central sleep apnea is worth understanding, particularly if you’re a CPAP user who’s noticed central events in your therapy data and isn’t sure what they mean. I should say clearly upfront: I don’t have central sleep apnea myself, I have obstructive, and nothing in this article is medical advice. I’m a patient who has read about this at length and spoken to people who live with it, not a clinician. Please take anything health-related here to a qualified doctor.
The Fundamental Difference
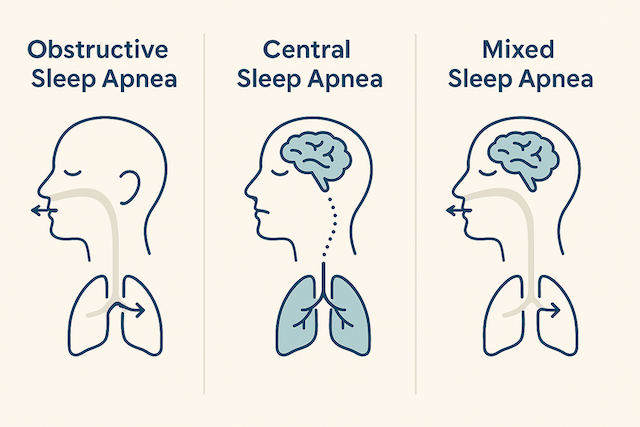
With obstructive sleep apnea, the problem is mechanical. The soft tissue in the throat relaxes during sleep, the airway collapses inward, airflow stops. Your brain detects the oxygen drop, forces a partial awakening, the airway reopens, and the cycle repeats. CPAP solves this by maintaining air pressure that physically prevents the airway from collapsing.
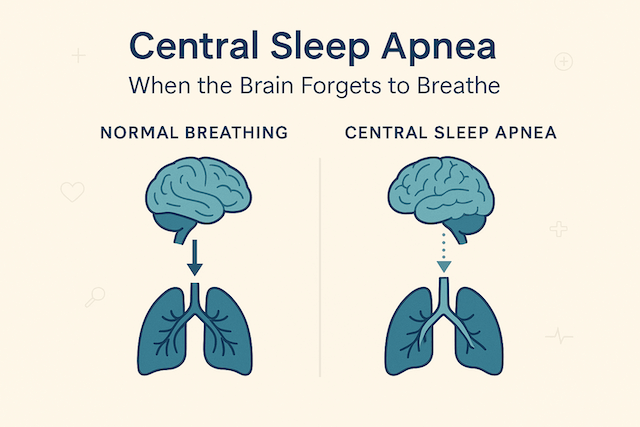
Central sleep apnea is entirely different. The airway is open. There’s nothing blocking it. The problem is that the brain simply doesn’t send the signal to breathe. The lungs are ready, the airway is clear, but the command never arrives. Breathing stops not because of a blockage but because of a communication failure between the brain and the respiratory muscles.
The consequence, an apnea event with dropping oxygen, looks similar on a sleep study to an obstructive apnea. But the cause is neurological rather than mechanical, and that distinction matters enormously for how it’s treated. CPAP alone, which is brilliant at solving the physical collapse problem, doesn’t necessarily address the signalling problem that causes central apneas.
What’s Actually Happening in the Brain
The breathing control mechanism that fails in central sleep apnea is normally elegant and automatic. Your brainstem monitors the level of carbon dioxide in your blood and uses it as the trigger to breathe. When CO₂ rises, you inhale. When you’ve inhaled and CO₂ drops, breathing pauses briefly until it builds back up. Under normal circumstances this balance is stable and you never notice it happening.
In people with central sleep apnea, that balance is unstable. The most common pattern is one of overshooting: the person breathes too deeply, which drops CO₂ too far too fast, and then the brain fails to restart breathing until CO₂ has climbed back to the trigger point. This creates a rhythmic pattern of heavy breathing followed by silence, which in its most distinctive form is called Cheyne-Stokes respiration. I wrote about Cheyne-Stokes respiration separately if you want more detail on that specific pattern, which is particularly associated with heart failure.
The instability of the system can have several different underlying causes, which is part of what makes central sleep apnea a more complex topic than obstructive sleep apnea. It’s not one thing with one fix.
Who Gets Central Sleep Apnea and Why
Central sleep apnea is considerably rarer than obstructive sleep apnea. It affects a small percentage of the general population but is significantly more common in specific groups, which points toward its causes.
Heart failure is one of the strongest associations. When the heart isn’t pumping efficiently, fluid can affect lung function and CO₂ regulation in ways that destabilise the breathing control system. The relationship runs in both directions, with the sleep disruption from central apnea putting additional strain on a heart that’s already compromised.
Neurological conditions are another significant category. Anything that affects the brainstem or the neural pathways involved in breathing control can potentially cause or contribute to central sleep apnea. Stroke is one example. Some structural abnormalities at the base of the skull, such as Chiari malformations where tissue presses on areas controlling breathing, can also be factors.
Opioid medications are a third major cause that I’ve read about extensively, partly because it’s one of the more practically important ones for people to know about. Opioids suppress the brainstem’s respiratory drive, and central sleep apnea is a recognised side effect of opioid use even at relatively low doses. This is relevant for anyone who starts opioid-based pain management and notices changes in how they sleep or how they feel on waking.
High altitude is a milder and usually temporary cause, as reduced oxygen at altitude can produce a similar overshooting pattern to what happens pathologically in CSA.
And then there’s what’s called treatment-emergent central sleep apnea, which is something a significant number of CPAP users encounter. This is where someone starts CPAP for obstructive sleep apnea and their therapy data begins showing central events that weren’t there before, or weren’t prominent before. The current understanding is that solving the obstructive problem can sometimes unmask a central component that was happening alongside it but wasn’t visible. In many cases treatment-emergent central apnea resolves on its own within a few weeks as the body adjusts to therapy. In some cases it persists and needs a different approach.
What It Feels Like to Live With It
Because I don’t have central sleep apnea myself, I’m drawing here on what I’ve heard from readers and CPAP community members who do. The consistent thing they describe is a particular kind of frustration that people with straightforward obstructive sleep apnea don’t usually encounter: doing everything right with their therapy and still not feeling well.
Someone with obstructive sleep apnea who uses their CPAP correctly and gets their AHI down generally starts feeling better fairly quickly. The therapy works. With central sleep apnea, particularly when it’s linked to heart failure or neurological conditions, the picture is murkier. The CPAP data might look confusing. The fatigue might persist. The sense that the therapy isn’t doing what it’s supposed to do can be demoralising.
People also describe less of the classic loud snoring and witnessed gasping that brings obstructive sleep apnea to attention in the first place. Central apnea is quieter. The person beside you might not notice anything alarming. You just wake up tired, morning after morning, without an obvious explanation.
The symptoms that come up most consistently are exhaustion that persists despite therapy, waking in the night short of breath or with a racing heart, morning headaches, and fragmented sleep that doesn’t feel restorative. If you’re a CPAP user and your machine is showing central apnea events alongside or instead of obstructive ones, it’s worth bringing that data to your sleep specialist rather than assuming it will sort itself out.
How It’s Diagnosed
The key diagnostic distinction in a sleep study is whether there is breathing effort during an apnea event. In obstructive sleep apnea, the chest and abdomen continue moving during the apnea because the person is trying to breathe against a blocked airway. In central sleep apnea, there is no movement at all. The airway is open but no effort is being made.
Modern sleep labs measure this through belts around the chest and abdomen that detect respiratory effort, alongside the airflow sensors and oxygen monitoring that capture the event itself. The combination tells the clinician not just that breathing stopped but why it stopped.
The Sleep Foundation’s overview of central sleep apnea is one of the clearer lay explanations of how this distinction is made and what the diagnostic process involves, and is worth reading if you want more detail than I can usefully provide as a non-clinician.
Where there’s uncertainty about the cause of central events, or where the condition is severe or not responding to standard therapy, doctors may also look at cardiac function, review medication lists, or consider neurological imaging. The treatment-emergent case I mentioned above, where a woman’s persistent central events eventually led to imaging that revealed a structural abnormality, is a reminder that not all central apnea has a straightforward explanation, and that it’s worth pursuing if it’s not resolving.
Treatment
Because central sleep apnea has different causes and different mechanisms to obstructive sleep apnea, treatment is correspondingly varied.
For treatment-emergent central apnea that appears after starting CPAP, watchful waiting with good data monitoring is often the first step, since many cases resolve spontaneously. Where it persists, adaptive servo-ventilation, known as ASV, is the most sophisticated response. An ASV machine monitors each breath in real time and adjusts its pressure support on a breath-by-breath basis, delivering a backup breath when one doesn’t come on its own. It’s the gold standard for moderate to severe CSA and particularly for the Cheyne-Stokes pattern. The important caveat, which any clinician prescribing it should be aware of, is that ASV is not appropriate for all heart failure patients, specifically those with significantly reduced ejection fraction, following findings from a trial called SERVE-HF.
BiPAP in a spontaneous-timed mode is another option, which provides a mandatory backup breath if the person doesn’t breathe within a set time window. For some patients supplemental oxygen helps stabilise the CO₂ balance sufficiently to reduce events. And where the central apnea has an identifiable underlying cause, treating that cause, optimising cardiac function in heart failure, adjusting or changing opioid medications where possible, can sometimes resolve or significantly reduce the sleep apnea alongside it.
The Practical Takeaway for CPAP Users
If you’re an obstructive sleep apnea patient on CPAP and you’re reading this because your machine data shows central events, the most useful thing I can tell you from everything I’ve read is not to either panic or dismiss it. A small number of central events in an otherwise clean night is often not clinically significant. A consistently elevated central apnea index, particularly if you’re also still feeling unwell despite good compliance, is worth a proper conversation with your sleep specialist and your GP.
The data your machine produces, particularly if you’re looking at it through something like OSCAR software which gives you the full picture rather than just the summary score, will show you the pattern. Bringing that data to your appointments rather than describing your symptoms from memory is one of the most useful things you can do to help your care team understand what’s happening.
Central sleep apnea is less common than obstructive sleep apnea, more varied in its causes, and in some ways more complex to manage. But it’s not untreatable, and for most people who encounter it as a component of their therapy data rather than as a standalone diagnosis, it’s a manageable part of the picture rather than a reason to lose confidence in the treatment path they’re on.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).