Can You Reverse Sleep Apnea Naturally? 🌿

When I was diagnosed in 2014, I asked my sleep specialist exactly this question. I was 51 events per hour — severe — and the idea of wearing a mask every night for the rest of my life felt overwhelming. Surely, I thought, there was something I could do. Some changes I could make. Some way out.
She was honest with me. For some people, yes — particularly those with mild sleep apnea driven primarily by weight or sleep position — lifestyle changes can reduce events per hour enough that the condition resolves or no longer requires treatment. For people with severe OSA like mine, lifestyle changes matter but they’re unlikely to eliminate the underlying problem. The anatomy, the muscle tone, the way the airway collapses dozens of times an hour — CPAP addresses that in a way that diet and exercise alone can’t.
I went away and did everything anyway. I lost 20 kilograms over the following year. I changed my sleep position. I cut alcohol during the week. My pressure came down and my AHI scores improved. But I still use my machine every single night, over a decade later, and I expect I always will. My case isn’t a failure — it’s just the honest reality for most people with severe obstructive sleep apnea.
What follows is a clear-eyed look at what the evidence actually supports: which interventions make a real difference, who they’re most likely to help, and what to expect if your OSA is on the more severe end of the spectrum. I’ll be specific about what I’ve tried personally and where I’m drawing on research rather than experience.
If you’re not sure whether you have sleep apnea or haven’t been tested yet, that should come before any of the below. A home sleep test can give you a clinically valid result within a few days without a clinic visit.
The Honest Answer Upfront
The Sleep Foundation’s overview of home remedies for sleep apnea puts it well: people with mild OSA may find that lifestyle changes significantly reduce or even eliminate symptoms, but moderate to severe cases typically need medical intervention. Lifestyle changes work best as an adjunct to treatment rather than a replacement for it.
The reason for this comes down to what’s actually causing your airway to collapse. For some people it’s primarily excess weight pressing on the airway, and losing that weight can make a significant physical difference. For others it’s anatomical — the way the jaw sits, the size of the soft palate, the muscle tone of the throat — and no amount of lifestyle change will alter the underlying structure enough to resolve the problem at the level of events per hour. Knowing which situation you’re in requires a sleep study, not a guess.
Weight Loss
This is the intervention with the strongest evidence behind it, and it’s the one I have the most direct experience with. Excess weight around the neck and upper body narrows the airway and makes it more prone to collapse during sleep. Losing a meaningful amount of weight can genuinely reduce the mechanical obstruction.
Research published in the American Journal of Respiratory and Critical Care Medicine found that losing 10 to 15 percent of body weight could reduce OSA severity by around half in some patients. My own experience was consistent with this — my AHI data improved as I lost weight, and my required pressure came down. What it didn’t do was cure my sleep apnea. At severe levels, the improvement was real but not sufficient to eliminate the need for treatment.
If your OSA is mild to moderate and weight is a contributing factor, this is genuinely the first place I’d focus. The effects compound over time, and unlike most other interventions it benefits your health across the board regardless of what it does to your sleep apnea specifically.
Sleep Position

This one surprised me in how significant the effect was when I paid attention to my nightly data. Sleeping on your back allows the tongue and soft palate to fall backward under gravity, partially or fully blocking the airway. Over half of OSA patients have what’s called positional sleep apnea, where symptoms are meaningfully worse in the supine position.
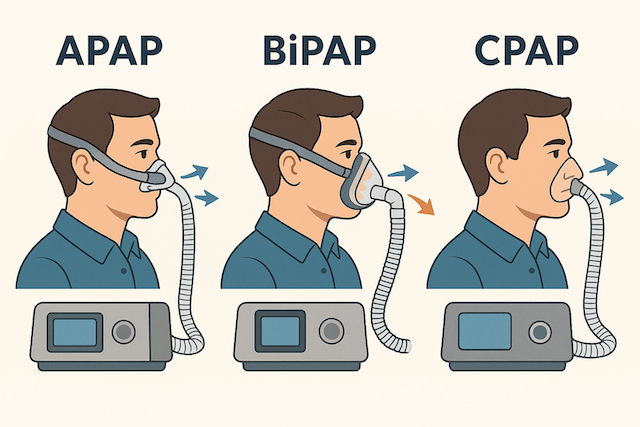
I can see this clearly in my own APAP data. Nights where I end up on my back — which happens more when I’m overtired and rolling around — consistently show higher event counts than nights where I stay on my side. For people whose OSA is predominantly positional, this is actually one of the more powerful things you can address.
Staying on your side through the night is easier said than done when you’re asleep, but a CPAP-specific pillow with the right shape helps significantly — both by making side sleeping more comfortable for CPAP users and by making it harder to roll comfortably onto your back. I’ve been using one for years and it’s made a consistent difference to my positional data.
Alcohol
This was the change that produced the most immediate and legible difference in my data. Alcohol relaxes the throat muscles, and relaxed throat muscles collapse more readily during sleep. Even one or two drinks a few hours before bed consistently pushed my events per hour upward — clearly enough that I could identify drinking nights from my myAir scores without thinking about it.
I cut evening alcohol during the week several years ago, partly for other reasons and partly because the data was so unambiguous. The effect is well documented — the Mayo Clinic’s guidance on sleep apnea treatment specifically lists avoiding alcohol as one of the first behavioural steps, alongside weight loss and sleep position. Cutting off at least 3 hours before bed is the standard recommendation; I ended up stopping altogether in the evenings.
Throat and Tongue Exercises
This one I’ll be honest about — it’s supported by evidence I find genuinely compelling, but it’s not something I’ve done with enough consistency to personally vouch for. A randomised controlled trial published in the American Journal of Respiratory and Critical Care Medicine found that daily oropharyngeal exercises — tongue presses, soft palate stretches, specific throat movements — reduced AHI by around 39% in people with moderate OSA and also reduced neck circumference and snoring intensity.
The mechanism makes sense: strengthening the muscles that support the upper airway reduces how readily they collapse during sleep. The difficulty is that “do specific mouth exercises every day” is a harder habit to build than “sleep on your side,” and compliance in practice tends to be lower than in clinical trials. If you’re motivated and consistent, the evidence supports giving this a proper try — at least eight to twelve weeks of daily practice before assessing results. I’ve reviewed a structured programme specifically built around this approach in my Stop Snoring and Sleep Apnea Program review, which is worth reading if you want a guided framework rather than piecing the exercises together yourself.
Smoking and Nasal Congestion
Smoking inflames and irritates the tissues lining the airway, increasing resistance and worsening obstruction. The evidence linking smoking to OSA severity is clear, and quitting is one of the better things you can do for both your sleep and your cardiovascular health simultaneously. I don’t smoke, so I have no personal experience here, but the mechanism is straightforward and well supported.
Nasal congestion is worth taking seriously even if it seems minor. If your nose is blocked, you default to mouth breathing, which bypasses some of the airway support that nasal breathing provides and can worsen obstruction. Regular saline rinses, proper allergy management, and ensuring your CPAP humidifier is calibrated for your climate all help keep your nasal passages clear overnight.
Mandibular Advancement Devices

These deserve mention as a genuinely evidence-based option, particularly for people who cannot tolerate CPAP or whose OSA is mild to moderate. A mandibular advancement device holds the lower jaw slightly forward during sleep, which physically prevents the tongue from falling back and blocking the airway.
The American Academy of Sleep Medicine includes these devices as an approved first-line therapy for mild to moderate OSA and as an alternative for people who prefer them to CPAP. They’re not as effective as CPAP at high severity levels, and they need proper fitting by a sleep dentist rather than relying on an over-the-counter boil-and-bite version — though those can work as a starting point to see whether the approach suits you. I’ve put together a full guide to the best sleep apnea mouth guards covering both custom-fitted and over-the-counter options with the specific differences explained, which is the right starting point if you’re considering this route.
What Natural Changes Won’t Do
They won’t reverse the anatomy. If your airway collapses because of the structure of your jaw, the size of your tonsils, or the length of your soft palate, no amount of weight loss or sleeping position adjustment will change the underlying architecture. Surgery can address some of these factors, but that’s well beyond the “natural” category.
They also won’t reliably control severe OSA to the degree needed to protect your cardiovascular health. The reason untreated severe sleep apnea is dangerous — the blood pressure, the heart strain, the long-term cardiovascular risk — is the cumulative effect of hundreds of oxygen desaturation events per night. Getting that number from 51 to 30 is meaningful, but it doesn’t get you to the under-5 threshold that represents properly controlled therapy. That’s what CPAP does.
What natural changes can do, even when they don’t eliminate the need for treatment, is improve how well your treatment works. My pressure is lower than it was at diagnosis. My compliance is easier. My overall health, partly because of the lifestyle changes I made, is genuinely better. The CPAP and the lifestyle changes work together — they’re not alternatives to each other.

If you’ve already made significant lifestyle changes and want to know whether your sleep apnea severity has actually shifted, a home sleep test is the right way to find out. It’s what I’d do rather than assuming the changes have been enough.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).