Sleep Apnea and Stroke Risk: What the Research Shows
I have severe obstructive sleep apnea. My AHI was 51 when I was diagnosed, which sits well inside the severe range, and I have lived with the condition for more than a decade. For a long time, I assumed sleep apnea was mostly about snoring and waking up tired. It took some reading before I understood that the breathing interruptions doing all that damage to my sleep were also putting strain on my cardiovascular system, including the blood vessels that feed my brain.
That changed how seriously I took therapy. This was no longer only about feeling less foggy during the day. It was about lowering the odds of a serious, possibly fatal stroke down the line.
I want to be clear about what this article is and is not. My background is in computer science, not medicine. I am a patient and a blogger, not a clinician, so nothing here is medical advice. What follows is what I have learned from living with this condition and from reading the research on how sleep apnea and stroke are connected. If you want the full story of how I got diagnosed and what the early years were like, that lives on my living with sleep apnea page. This piece stays focused on the stroke question.
What the research actually says
The link between sleep apnea and stroke is not a fringe idea. It shows up consistently in large studies published in major medical journals.
One of the most cited is a study from the New England Journal of Medicine that followed patients with obstructive sleep apnea over several years. After accounting for other risk factors such as high blood pressure, diabetes, and high cholesterol, the researchers found that obstructive sleep apnea was independently associated with roughly a twofold increase in the risk of stroke or death from any cause. You can read the study summary directly from the New England Journal of Medicine.
The relationship also runs the other way. When researchers look at people who have already had a stroke, a strikingly large share of them turn out to have sleep apnea, often undiagnosed until after the stroke happened. The same body of research notes that sleep apnea is present in more than 60 percent of stroke patients, compared with a much smaller fraction of the general middle aged population. That number is one of the things that made me stop treating my CPAP machine as optional.
Severity appears to matter too. The general pattern in the research is that people with severe disease carry a higher stroke risk than those with mild or moderate disease. The standard way clinicians grade severity is the apnea-hypopnea index, or AHI, which counts how many times per hour your breathing stops or becomes too shallow. Under 5 is considered normal, 5 to 14 is mild, 15 to 29 is moderate, and 30 or higher is severe. At 51, I was firmly in the severe group, which is part of why my doctor was so insistent about starting treatment quickly.
Why sleep apnea raises stroke risk
The connection is not a single mechanism. Researchers have identified several ways that untreated obstructive sleep apnea wears down the cardiovascular system over time. Understanding them helped me see why this is a quiet, cumulative problem rather than something you would feel happening.
Repeated oxygen drops strain the blood vessels
Each time the airway collapses during sleep, oxygen levels in the blood fall. This is called intermittent hypoxia. The drops are brief, but with severe apnea they happen again and again all night, and the research suggests that over months and years this pattern damages the lining of blood vessels throughout the body, including those supplying the brain. The damage tends to make vessels stiffer and narrower, which is exactly the kind of change that raises stroke risk.
Blood pressure surges put the system under stress
When breathing stops, the body responds with a burst of stress hormones to rouse you just enough to start breathing again. Heart rate and blood pressure spike with each event. Repeated night after night, this is thought to contribute to chronic high blood pressure, particularly raised pressure at night, which is one of the stronger predictors of stroke. The Mayo Clinic explains the cardiovascular strain side of this clearly in its overview of obstructive sleep apnea.
Inflammation and plaque buildup
Untreated sleep apnea is also associated with low grade, ongoing inflammation in the body. That inflammation feeds atherosclerosis, the buildup of plaque inside the arteries. When plaque accumulates in the arteries that carry blood to the brain, the risk is that a piece breaks loose or blocks flow entirely, which can cause an ischemic stroke, the most common type. This process can be progressing silently even when you feel fine during the day.
Irregular heart rhythm and clots
Sleep apnea is linked to a higher risk of atrial fibrillation, an irregular heart rhythm. When the heart beats irregularly, blood can pool and form clots, and a clot that travels to the brain can cause a stroke. I dug into this more in my piece on sleep apnea and cardiovascular health. The encouraging part is that research suggests treating the apnea can reduce how often atrial fibrillation recurs.
The part that gave me some relief
Reading all of this was unsettling at first. I had gone in thinking I snored loudly and woke up tired, and came out understanding that the condition carried real cardiovascular stakes. What steadied me was noticing that almost all of the risk in the research applies to untreated sleep apnea.
Studies of people who use CPAP consistently tend to show better cardiovascular outcomes than those who go untreated, including lower rates of fatal and nonfatal cardiovascular events. More recent analyses point in the same direction, with the important caveat that the benefit depends on actually using the machine. Adherence is the word that comes up over and over. Research generally points to using CPAP at least four hours a night to see cardiovascular benefit, with more being better. Wearing it most nights helps. Wearing it every night helps more.
That framing is what keeps me consistent on the nights I would rather not bother. I am not only chasing better sleep. I am trying to protect my heart and brain over the decades ahead.
What treatment has looked like for me
I am a chronic mouth breather, which rules out nasal masks for me, so I use a full face mask. My main machine is a ResMed AirSense 10, which I have used for the better part of a decade, and I keep a smaller ResMed travel unit for trips and camping so that therapy does not stop when I leave home.
The early weeks were not smooth. The mask felt strange, I dealt with dry mouth, and I had a fair amount of anxiety about sleeping with the thing on my face. What got me through was treating it as a skill to learn rather than a verdict on whether I could cope. One genuinely good change that I can point to from my own experience is that the morning headaches and migraines I used to wake up with eased off after I started therapy. That was the first sign for me that the machine was doing something real.
I track my therapy through the myAir app and check my numbers regularly. If staying consistent is the hard part for you, that is normal, and I put together some of what helped me in a piece on staying consistent with CPAP therapy.
Recognizing the warning signs
One thing that struck me is how many sleep apnea symptoms overlap with reasons to take cardiovascular risk seriously. Loud, chronic snoring is often the first thing a partner notices. Gasping or choking during sleep is another. So are heavy daytime fatigue even after a supposedly full night, morning headaches, trouble concentrating or remembering things, and mood changes or irritability.
Looking back, I had most of these and chalked them up to stress and getting older. The reality was that my breathing was being interrupted dozens of times an hour. If any of this sounds familiar, it is worth reading through the fuller list of sleep apnea symptoms and raising it with a doctor rather than waiting it out the way I did.
Getting diagnosed
The standard way to diagnose sleep apnea is a sleep study, which measures breathing, oxygen levels, heart rate, and other signals while you sleep. These days a lot of testing can be done at home with portable equipment rather than an overnight lab stay. I was diagnosed using an at home sleep test myself. If you want to understand what the testing process involves and how the results are read, I cover that in my overview of the diagnosis process. A study can also distinguish obstructive sleep apnea from other forms of the condition, which matters because the right treatment depends on which type you have.
Lowering your risk beyond the machine
CPAP is the front line treatment for most people with obstructive sleep apnea, but it is not the only lever. The research consistently points to a handful of lifestyle factors that affect both apnea severity and stroke risk.
Weight is one of the biggest. Studies have found that even modest weight loss can lower AHI and improve overnight oxygen levels. I have written separately about the relationship between CPAP therapy and weight, since the two tend to influence each other.
Smoking is another. It damages blood vessels directly and worsens apnea by inflaming the airway, so a smoker with sleep apnea is stacking risk on top of risk. Alcohol is worth watching as well, because it relaxes the airway muscles and can make apnea events worse, which is why a lot of guidance suggests keeping it away from the hours close to bedtime. Regular physical activity rounds out the list, with some research suggesting exercise can reduce apnea severity even independently of weight loss.
None of these replace treatment, but together they shift the odds in your favor.
Different groups, different patterns
Sleep apnea does not present the same way for everyone, and that affects who gets diagnosed in time.
Women are often underdiagnosed because the symptoms can look different. Rather than the classic loud snoring and obvious pauses, women may report insomnia, morning headaches, and low mood, which are easier for a clinician to attribute to something else. The stroke risk, though, is comparable. If that describes your experience, it is worth pushing for a proper sleep study rather than accepting a quick dismissal. I go into this more in my piece on sleep apnea in women.
Older adults are another group where this matters a great deal, since both sleep apnea and stroke risk climb with age and often sit alongside other conditions like high blood pressure and diabetes. And there is a notable overlap after stroke itself: a large share of stroke survivors have sleep apnea, sometimes worsened by the stroke, which is why screening for it is increasingly treated as part of recovery and prevention of a second event.
If you cannot tolerate CPAP
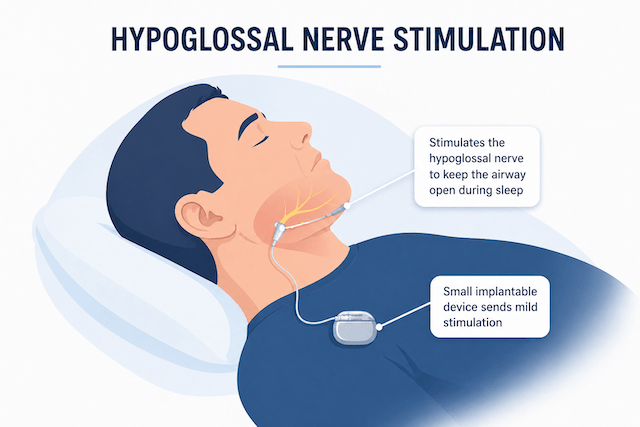
CPAP is effective, but not everyone gets on with it, and an untreated airway is the worst outcome. Several alternatives exist depending on the severity of your apnea and your anatomy. Oral appliances can help with mild to moderate cases by holding the jaw forward. Various surgical procedures address physical obstructions. Hypoglossal nerve stimulation is an implantable option for selected patients. And for people whose apnea is much worse on their back, positional therapy can sometimes reduce AHI. The right path is a conversation for you and your sleep doctor, but the goal is always the same: keep the airway open and the oxygen steady.
The bottom line
Here is what more than a decade with this condition, and a lot of time spent reading about it, has left me with. The link between sleep apnea and stroke is well supported across major medical journals, and it runs through several mechanisms at once: repeated oxygen drops, blood pressure surges, inflammation, and irregular heart rhythm. That is the sobering half.
The reassuring half is that treatment changes the picture. Consistent CPAP use is associated with meaningfully lower cardiovascular risk, and lifestyle changes add to that. The benefit comes from actually using therapy, night after night, which is the part only you can do.
When I first started CPAP I was mostly motivated by wanting to feel less exhausted. These days the bigger reason is wanting to be around and healthy for a long time. If you have symptoms, get tested. If you have been diagnosed and the machine is gathering dust, it is worth another honest attempt, ideally with your doctor helping you sort out whatever made it hard the first time.
Frequently asked questions
Can CPAP reverse damage from a stroke?
No. CPAP does not undo damage that has already happened. What the research suggests is that treating sleep apnea after a stroke may support better recovery and lower the risk of a second stroke, which is a different and still worthwhile benefit. Follow your own doctor’s guidance for your situation.
Should I keep using CPAP after a stroke?
For most people in that situation, it becomes more important, not less. Many stroke survivors either already have sleep apnea or develop it afterward, and continuing therapy helps keep oxygen levels steady and blood pressure in check. This is something to confirm with the clinician managing your recovery.
What about mini strokes, or TIAs?
The research links sleep apnea with a higher likelihood of transient ischemic attacks, and untreated apnea raises the chance that warning events progress to a full stroke. If you have had a TIA, getting screened and treated for sleep apnea is worth prioritizing.
I feel fine during the day. Do I really need treatment?
This was my own assumption for a long time. The catch is that the cardiovascular damage from untreated apnea accumulates quietly, whether or not you feel impaired, and many people with severe disease have simply adapted to functioning on poor sleep. Feeling okay is not the same as being in the clear.
Does sleep position affect any of this?
Sleeping on your back tends to worsen apnea, because gravity lets the tongue and soft tissue fall back and block the airway. Positional therapy can reduce AHI for people whose apnea is position dependent. CPAP, by contrast, works regardless of position, which is part of why it remains the more reliable option.
How quickly does treatment help?
Some benefits, like improvements in blood pressure, can show up within weeks to months of consistent use. The cardiovascular protection seen in longer studies builds up over years of steady therapy. Consistency is the thread running through all of it.
One last thing. Please do not take my word as medical advice. I am not medically trained. I share my own experience and what I have read, and the right plan for you is one you work out with a qualified clinician.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).