Sleep Apnea Diagnosis – Understanding the Condition
This picture represents me. I was happy when I received my sleep apnea diagnosis because it answered all the questions I had about my headaches and migraines.
If you have ever woken up gasping in the middle of the night, or your partner has nudged you awake because you stopped breathing, you already know something is wrong. The hard part is getting an answer. A sleep apnea diagnosis is the bridge between “I think something is going on with my sleep” and “I now have a plan that can give me my life back.”
I was diagnosed with severe obstructive sleep apnea more than a decade ago. My AHI came back at 51, which sits well into the severe range. My wife pushed me to get tested after watching me gasp and stop breathing too many times to ignore. I share more about that personal journey on my Living with Sleep Apnea page. This page is different. This is the practical guide I wish I had read before I made that first appointment.
A quick note before we start. I am a CPAP user with a computer science background, not a doctor. The information here is meant to help you understand what diagnosis looks like and what questions to ask your clinician. It is not a substitute for medical advice from someone qualified to give it.
What Sleep Apnea Actually Is
Sleep apnea is a sleep disorder where your breathing repeatedly stops and starts during the night. Each pause might last only a few seconds, but in moderate or severe cases it happens dozens of times an hour. Your brain pulls you partly out of sleep each time so you can breathe, which is why you feel exhausted the next day even after what looked like a full night in bed.
Doctors recognize three forms of the condition. Obstructive Sleep Apnea, or OSA, is by far the most common and is caused by the soft tissue in the throat collapsing and blocking the airway. Central Sleep Apnea is rarer and happens when the brain stops sending the normal signals telling the body to breathe. Complex or mixed sleep apnea involves features of both. The type matters because it changes the treatment.
Untreated sleep apnea is not just a snoring nuisance. It is associated with high blood pressure, heart disease, type 2 diabetes, stroke, depression, and a higher risk of crashes from drowsy driving. The American Academy of Sleep Medicine and clinical centers like Mayo Clinic treat it as a chronic disease that needs a real diagnosis and ongoing follow up. That is why this step matters so much.
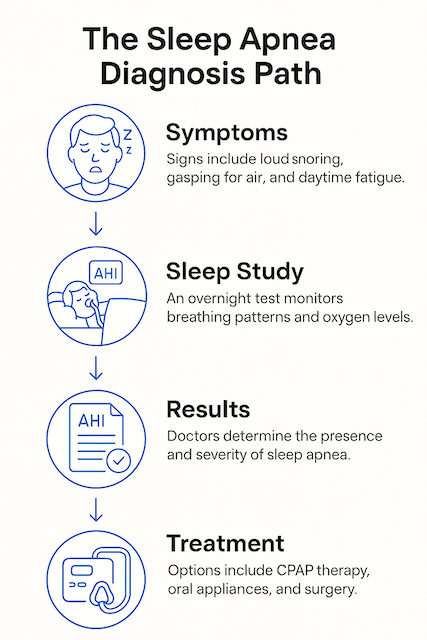
Symptoms That Should Push You Toward Testing
Sleep apnea is one of those conditions where the person who has it is often the last to notice. You are asleep when the worst of it is happening. The signs that finally bring most people to a clinic tend to come from a partner.
Loud, persistent snoring is the obvious one. Pauses in breathing followed by gasping or choking sounds are more telling. Waking up with a dry mouth, a sore throat, or a morning headache shows up often. So does daytime exhaustion that does not respond to caffeine, mood changes, brain fog, and the sense that you can fall asleep on the couch the moment any episode of anything starts playing.
Some people brush this off as the price of getting older, working too hard, or carrying a few extra pounds. I did the same for years. The cost of that delay was worse than I realized at the time. I was getting crushing migraines that I now believe were tied directly to oxygen drops at night.
If your partner has counted long pauses in your breathing, that alone is enough reason to make an appointment. They do not have to be 30 second pauses to matter. Quiet stretches followed by sudden snorts or gasps are exactly the pattern doctors look for.
Risk Factors That Increase Your Odds
You can have sleep apnea without any of the classic risk factors, and many slim, fit people are surprised by their diagnosis. That said, certain things raise your probability enough that doctors take symptoms more seriously when they show up alongside them.
Being overweight is the largest single risk factor for OSA. Extra tissue around the neck and upper airway makes collapse more likely when the muscles relax in sleep. Neck circumference matters as much as overall weight here. Age is a factor, since muscle tone in the throat decreases over time. Men are diagnosed more often than women, though women are likely underdiagnosed because their symptoms can present differently. A family history of sleep apnea, smoking, alcohol use in the evening, and chronic nasal congestion all push the needle. Anatomical features such as a recessed jaw, a large tongue, or enlarged tonsils contribute as well. Doctors sometimes use the Mallampati score, a quick visual exam of how much of the back of your throat is visible when you open your mouth, to estimate airway crowding.
The Two Paths to a Sleep Apnea Diagnosis
There is also a strong link between sleep apnea and conditions like high blood pressure, type 2 diabetes, atrial fibrillation, and stroke. The relationship runs both ways. Sleep apnea can worsen these conditions, and these conditions are often where doctors first start asking about sleep.
Modern sleep apnea diagnosis usually goes one of two ways. You will either spend a night in a sleep lab, or you will sleep at home with a small kit on your chest and finger. Both paths end with a report that includes your AHI score and enough detail for a sleep doctor to recommend a treatment plan.
Polysomnography, the In Lab Sleep Study
Polysomnography is the gold standard. According to the American Academy of Sleep Medicine’s clinical practice guideline, it remains the reference test for diagnosing OSA in patients, where home testing might miss something important.
Here is what actually happens. You arrive at the sleep center in the evening, get checked in, and are taken to a private room that is meant to feel as much like a bedroom as a clinical setting allows. A technologist places sensors on your scalp, face, chest, and legs. There are a lot of wires, but they are designed to be tolerable enough to sleep with. The sensors record brain activity, eye movements, heart rhythm, breathing effort, airflow at the nose and mouth, blood oxygen, snoring intensity, body position, and limb movements.
You sleep, or try to. Most people are convinced they barely slept and the technologist still gets enough usable data to score the night. The morning after, you go home. A few weeks later you sit down with the doctor, who walks you through the report.
Lab studies are still the right call when you have heart or lung disease, suspected central sleep apnea, complex symptoms, possible narcolepsy or other parasomnias, or when home testing has come back inconclusive. They are also used for CPAP titration studies, where the goal is to figure out the right pressure setting for your therapy.
Read more here about what to expect if you take a Polysomnography (Lab Study) test
Home Sleep Apnea Tests
For the more common case of suspected moderate to severe OSA in an otherwise healthy adult, an at home sleep apnea test is now often the first step. The test usually involves a small device worn on the chest, a sensor at the finger or wrist, and a thin tube under the nose that measures airflow.
The trade off is straightforward. Home tests measure fewer things than a full lab study, but they record you in your own bed, in your own clothes, on your own pillow. For someone whose stress about being wired up in a strange room would itself ruin the data, that is a real benefit. The American Academy of Sleep Medicine endorses home testing for adults with a high probability of moderate to severe OSA and no major medical complications.
If a home test comes back negative but your symptoms are clearly there, the next step is usually an in-lab study. A negative home test is not always the final word, especially if a sensor came loose at 3 a.m.

If you want to read about a specific home test option, I have written about the WatchPAT One, which uses a slightly different sensor approach than the standard chest belt setup.
What Your AHI Score Actually Means
After your sleep study, the report will include an Apnea-Hypopnea Index, or AHI. This is the average number of breathing events you have per hour of sleep. An apnea is a complete pause in airflow, a hypopnea is a partial drop. Doctors typically use four categories. An AHI under 5 is considered normal, 5 to 14 is mild, 15 to 29 is moderate, and 30 or higher is severe. My number at diagnosis was 51, which translates to more than fifty breathing events every hour. No wonder I was tired.
The AHI is the headline number, but it is not the whole story. The report will also include oxygen saturation data showing how low your blood oxygen dropped during events, the time you spent in different sleep stages, and how often you actually entered REM sleep. Some people have a relatively modest AHI but very deep oxygen drops, and that combination can do real damage. A good clinician reads the whole report, not just the AHI.
The Conversation Before the Sleep Study
Before any test, your doctor will likely take a sleep history and ask you to fill out a screening questionnaire. The Epworth Sleepiness Scale is one of the most common. It asks how likely you are to doze off in eight everyday situations, from sitting and reading to stopped in traffic. The STOP-BANG questionnaire is another widely used screen that adds anatomical and demographic risk factors.
These tools cannot diagnose sleep apnea. They are filters. A high score helps your doctor decide that a sleep study is justified, and a low score does not rule the condition out if your symptoms are otherwise convincing. Mayo Clinic notes that a sleep test is the only way to confirm OSA, regardless of how the questionnaires score.
What Happens After You Get a Diagnosis
The diagnosis appointment was a strange experience for me. I was relieved more than alarmed. Years of unexplained fatigue and headaches finally had a label. The doctor told me I had severe OSA and recommended starting CPAP therapy as soon as possible.
For most people the conversation covers three things. First, the type and severity of sleep apnea you have. Second, the recommended treatment. Third, the follow up plan. With CPAP that follow up usually includes a fitting for a mask, an introduction to the machine and humidifier, and a return visit to download data from the device and see how the therapy is going.
I will be honest. The first few weeks of CPAP were not easy. I dealt with CPAP anxiety before I figured out how to settle in with the mask. I am a chronic mouth breather, so a full face mask was the right call from the start, and I have used a ResMed AirSense 10 for the better part of a decade. Once I got used to the therapy, the change was bigger than anything I had expected. The migraines eased. The brain fog lifted. I started waking up feeling something close to rested.
Treatment Options at a Glance
The right treatment depends on what type of sleep apnea you have, how severe it is, your anatomy, and your tolerance for different therapies.
CPAP therapy is the most common and most effective treatment for moderate to severe OSA. A small machine sits beside the bed, pulls in room air, and delivers a steady pressure through a hose and mask that keeps your airway open. There are alternative machines such as APAP, which adjusts pressure automatically, and BiPAP, which uses two pressure levels and is sometimes used when standard CPAP is not effective or not tolerated.
Oral appliances made by a sleep dentist can work for mild to moderate OSA. They reposition the lower jaw or tongue to keep the airway open. They are not a fit for everyone and they need follow up testing to confirm they are actually working.
Lifestyle changes do help. Weight loss when relevant, sleeping on your side, avoiding alcohol close to bedtime, and treating nasal congestion can all reduce events. There is some evidence that meaningful weight loss can improve or even resolve sleep apnea in milder cases, although it is not a quick fix and is not a reason to delay therapy in the meantime.
Surgical options include various airway procedures and, for selected patients, hypoglossal nerve stimulation devices. These are usually reserved for cases where positive airway pressure is not tolerated or has not produced the desired result.
Why Delaying Diagnosis Is Riskier Than People Realize
Sleep apnea is sneaky because the worst damage is silent and cumulative. You can convince yourself that being tired all the time is just how life is now, while in the background your cardiovascular system is paying for hundreds of oxygen dips every night.
The risks of leaving it untreated include high blood pressure, atrial fibrillation, heart attack, stroke, type 2 diabetes, and accidents tied to drowsy driving. There is also evidence that ongoing CPAP therapy may improve life expectancy compared with leaving severe OSA untreated. None of this is meant to scare you. It is meant to make the decision to get tested feel less like an inconvenience and more like a basic act of self care.
The flip side is also true. Treatment works. Most people who stick with CPAP report that they feel meaningfully different within weeks, and the longer term improvements in cardiovascular numbers, mood, and daytime function are well documented in the clinical literature.
A Quick Note on Children
Sleep apnea is not just an adult condition. Sleep apnea in children often presents differently than in adults. Instead of obvious daytime sleepiness, you might see hyperactivity, attention problems, poor school performance, bedwetting, or chronic mouth breathing. If you are a parent and these signs sound familiar, it is worth asking your pediatrician about a sleep study. The diagnostic tools are similar but the interpretation and treatment are best handled by a pediatric sleep specialist. I have a separate guide on whether your child might have sleep apnea if you want to read more.
Frequently Asked Questions
Can I diagnose sleep apnea on my own using a smartwatch or app? No. Consumer wearables and apps can flag patterns that suggest sleep apnea, and they have actually pushed many people to seek testing, which is a good thing. They are not, however, a substitute for a proper sleep study. Only an in lab polysomnogram or a clinically validated home sleep apnea test can confirm the diagnosis and produce a report your doctor can act on.
How accurate are home sleep apnea tests? For uncomplicated adults with a clear clinical picture of moderate to severe OSA, home tests are reliable and have been endorsed by the AASM as a reasonable first step. They are less suited to picking up central sleep apnea or to people with significant heart, lung, or neurological conditions. A negative home test in someone with strong symptoms usually triggers an in lab study.
How much does a sleep study cost? Costs vary widely by country, region, insurance, and whether the test is in lab or at home. In the United States, in lab studies typically run into the low thousands of dollars before insurance, and home tests are usually a fraction of that. Many insurance plans cover home testing first because it is cheaper. The most reliable answer is to call your insurer or sleep clinic directly and ask for an estimate.
Will I be able to sleep with all those wires on me? Almost everyone is convinced they barely slept during their study. Almost everyone gets enough usable data anyway. The technicians are very good at getting what they need from imperfect nights.
How often do I need to be retested after diagnosis? Most people on stable CPAP therapy do not need a repeat full study unless their symptoms change, they lose or gain a significant amount of weight, they switch treatments, or their CPAP data shows the therapy is no longer controlling events. Periodic CPAP data downloads usually replace the need for repeat sleep studies.
Should I push for an in lab study even if my doctor recommends a home test? Not necessarily. The home test path is appropriate for many people and is faster, cheaper, and more comfortable. Where you should push back is if the home test is negative but you and your partner are convinced something is still going on at night. That is exactly the case for moving to a full polysomnogram.
Final Thoughts
Getting tested feels like a hassle. It is not. It is one night of mild inconvenience in exchange for an answer that can change everything that comes next. I waited too long because my symptoms grew slowly enough that I rationalized them away. Looking back, that delay cost me years of feeling worse than I needed to and probably did damage to my body that better sleep can only partly undo.
If your partner is poking you in the ribs at night, if you wake up with a headache more often than not, or if you are tired in a way that no amount of coffee fixes, please make the call. Ask your doctor about either a referral to a sleep specialist or an at home sleep apnea test as a first step. The hardest part of the whole process is making the appointment.
Once you have a diagnosis, you have options. From there it is a matter of finding the right treatment, the right mask if you go the CPAP route, and giving your body time to recover from years of underslept nights. My next recommended read is my guide to the Apnea-Hypopnea Index, which goes deeper into how doctors interpret your numbers.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).