CPAP vs BiPAP: Understanding the Differences

If you have just been diagnosed with sleep apnea, one of the first questions you run into is which machine you are actually supposed to use. Your doctor mentions a PAP machine, you start reading, and within an hour, you have seen CPAP, BiPAP, APAP, and a handful of other acronyms that all look interchangeable. They are not.
I have used a CPAP machine for more than a decade. It is, without exaggeration, the thing that gave me my days back after years of severe obstructive sleep apnea, so I can speak to CPAP from genuine experience. I want to be upfront about the other half of this comparison though. I have never used a BiPAP. Everything I say about BiPAP here comes from research and from what reputable medical sources and sleep specialists describe, not from my own nights of sleep. My background is in computer science, not medicine, so treat this as one patient’s guide to the landscape rather than a clinical recommendation.
That honesty matters here, because the choice between CPAP and BiPAP is not something you make on your own anyway. It is made with a sleep specialist, usually after a sleep study. What this article can do is help you walk into that conversation understanding what each machine does, who each one tends to suit, and why a doctor might steer you toward one over the other.
If you want a quick refresher on what all the acronyms mean before going further, I cover that in my what does CPAP stand for article.
What a CPAP Machine Does
CPAP stands for continuous positive airway pressure, and it is the most commonly prescribed therapy for obstructive sleep apnea. It is also the machine I use every night.
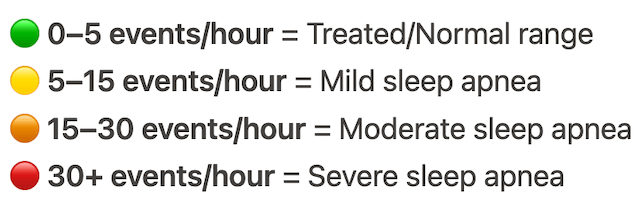
The idea behind it is simple. In obstructive sleep apnea, the soft tissue at the back of your throat relaxes and collapses while you sleep, briefly blocking your airway. You stop breathing, your body panics a little, you surface just enough to gasp air back in, and the cycle repeats. It can happen dozens of times an hour without you ever fully waking up enough to remember it. A CPAP machine deals with this by pushing a constant, steady stream of pressurized air through a hose and mask. That gentle pressure works like a splint, holding the airway open so it cannot collapse in the first place.
The key word is constant. A standard CPAP delivers the same pressure whether you are breathing in or breathing out. That single fixed pressure is set for you, usually based on a sleep study, and it does not change through the night.
CPAP works with whatever mask suits you. Some people use a nasal mask, some use nasal pillows, and some, like me, use a full face mask. I am a chronic mouth breather, so a full face mask was the obvious choice from the start. If air is going to escape through your mouth all night, a mask that covers only your nose is going to fight you.
There are good reasons CPAP is the default. It is highly effective for straightforward obstructive sleep apnea, it is generally the most affordable type of PAP machine, and it is the simplest to live with. Fewer settings means fewer things to misunderstand and fewer things to get wrong.
I will not pretend the first few weeks were effortless. Getting used to sleeping with a mask and a hose took real adjustment, and that early stretch was the hardest part of the whole process. I have written separately about getting past CPAP anxiety because that adjustment period deserves its own discussion. But once I was through it, the change was hard to overstate. I stopped waking up gasping. I stopped dragging myself through the day half awake. Years of sleep deprivation had a cause, and the machine finally addressed it.
What a BiPAP Machine Does
BiPAP stands for bilevel positive airway pressure. This is where the comparison gets interesting, and it is also the part I am describing as a researcher rather than a user.
The core difference is right there in the name. Where a CPAP delivers one pressure, a BiPAP delivers two. There is a higher pressure for when you breathe in, called IPAP (inspiratory positive airway pressure), and a lower pressure for when you breathe out, called EPAP (expiratory positive airway pressure). The machine switches between the two in time with your breathing.
Why does that matter? Because for some people, exhaling against a steady wall of pressurized air is uncomfortable. With a CPAP, you are breathing out against the same pressure that is helping you breathe in. Most people adjust to that without much trouble, and modern CPAP machines have softened it further with pressure relief features that ease off slightly as you exhale. But for a subset of people, particularly those who need high pressures or who have additional breathing conditions, that constant resistance is a genuine obstacle. A BiPAP drops the pressure when you exhale, so breathing out feels closer to natural.
According to the Sleep Foundation, BiPAP may be recommended over CPAP for people with more complicated breathing disorders, or in cases where CPAP is not controlling the sleep apnea effectively. It is also a common option for people who find exhaling against CPAP pressure too difficult to tolerate.
BiPAP also tends to be used beyond obstructive sleep apnea alone. It is often prescribed for central sleep apnea, which is a different problem altogether. There the airway is open, but the brain is not reliably sending the signal to breathe. BiPAP is also used for chronic respiratory conditions like COPD, where the lungs need extra support. Some BiPAP machines run on preset pressures while others can automatically adjust, and they generally offer a wider pressure range than a standard CPAP.
If you want a fuller breakdown of how BiPAP machines are built and used, I go deeper in my what is a BiPAP machine article.
The Practical Differences, Side by Side
Before we get into the detail, this short video from Sleep Doctor walks through the CPAP and BiPAP comparison if you would rather watch than read.
It helps to look at the two machines across the things that actually affect daily life.
Air pressure is the headline difference. CPAP gives you one pressure all night. BiPAP gives you two, splitting inhale and exhale. Almost everything else follows from that.
Comfort is where the split shows up for real people. Most users with straightforward obstructive sleep apnea do fine on CPAP, and many never feel the constant pressure as a problem at all. The people who struggle tend to be those on higher pressure settings, or those with conditions that make breathing harder to begin with. For them, the lower exhale pressure of a BiPAP can be the difference between tolerating therapy and abandoning it.
The conditions each machine treats differ too. CPAP is built around obstructive sleep apnea, and that is the overwhelming majority of cases. BiPAP covers obstructive sleep apnea as well, but it stretches further into central sleep apnea, COPD, and other situations where the lungs or the breathing drive need more support than a single pressure can give.
Cost is a real factor. BiPAP machines are generally more expensive than CPAP machines because of the added capability. Insurance coverage often depends on documented medical need, so a BiPAP is typically prescribed when there is a clear clinical reason for it rather than offered as a comfort upgrade.
Finally, complexity. CPAP machines are simple by design, with a fixed or automatically adjusting pressure and not much for the user to think about. BiPAP machines have more settings and more room for fine tuning, which is useful when breathing needs are complex but also means the setup matters more.
If you also want to see where APAP fits into all of this, since it is the third name people keep running into, I compare all three in my article on the difference between APAP, BiPAP, and CPAP. And for the more specialized end of the spectrum, there is also ASV, which I cover in ASV vs BiPAP vs CPAP.
When a Doctor Might Recommend BiPAP Over CPAP
CPAP is almost always the starting point for obstructive sleep apnea. But there are a few well recognized situations where a sleep specialist may move someone to BiPAP instead.
The most common is difficulty exhaling against CPAP pressure. When breathing out against the machine becomes a fight, people stop using the machine, and a therapy you do not use does nothing for you. The lower exhale pressure of a BiPAP removes that obstacle.
A second is high pressure requirements. Some people need a lot of pressure to keep the airway open. The higher the pressure, the harder it is to exhale against, so splitting the pressure into two levels makes those higher settings far more livable.
A third is a coexisting respiratory or breathing condition. If someone has central sleep apnea, COPD, or another condition that affects how they breathe, a single fixed pressure often is not enough. BiPAP gives the clinician more control to match the therapy to the problem.
The thread running through all of these is that BiPAP is not a better machine than CPAP. It is a different tool for a different job. The Sleep Foundation makes a point worth repeating: in recent years, the gap between the two has actually narrowed, because many modern CPAP machines now include pressure relief features that ease exhalation. For a lot of people, that closes the comfort gap before BiPAP ever enters the conversation.
A Note on Getting the Right Machine
I want to be clear about something, because it is easy to read a comparison like this and start shopping. You do not choose between CPAP and BiPAP the way you choose between two laptops.
Both CPAP and BiPAP machines are prescription medical devices. In the United States you cannot legally buy either one without a prescription, and I cover why in my article on whether you need a prescription for a CPAP machine. The prescription exists for a reason. The right machine, and the right pressure settings on that machine, come out of a sleep study and a clinician’s assessment. Guessing your way to the wrong therapy or the wrong pressure is not a shortcut, it is a way to spend money on something that does not treat your condition.
So if you are weighing CPAP against BiPAP, the most useful thing you can do is bring the question to your sleep specialist. Ask them directly why they are recommending what they are recommending. A good clinician will happily explain it. If you have been on CPAP and you are struggling specifically with exhaling, that is concrete, useful information to bring to them, because it is exactly the kind of problem BiPAP is designed to solve.
If you do reach the point of looking at specific BiPAP models, I have pulled together a research based overview in my best BiPAP machines guide.
Frequently Asked Questions
Is a BiPAP louder than a CPAP? Not as a rule. Modern machines of both types run quietly, and noise has more to do with the specific model and how well your mask is sealing than with whether it is a CPAP or a BiPAP. If machine noise is something you are sensitive to, I have written more about that in my piece on the quietest CPAP machines.
Can I buy a BiPAP without a prescription? In the United States, no. Both CPAP and BiPAP machines are classified as medical devices and require a prescription.
Is BiPAP better than CPAP? Better is the wrong frame. They are different tools. CPAP is the right fit for most people with obstructive sleep apnea. BiPAP becomes the better fit when CPAP is not enough, whether that is because of exhale discomfort, high pressure needs, or an additional breathing condition.
What if a BiPAP is recommended but I cannot afford it? Talk to your doctor and your insurer. Coverage often hinges on documented medical necessity, and if a BiPAP is genuinely needed, that necessity can usually be established. It is a conversation worth having rather than assuming the cost is fixed.
Will switching to BiPAP cure my sleep apnea? No machine cures sleep apnea. CPAP and BiPAP both manage it, and they only work on the nights you actually use them. They treat the condition. They do not remove it.
Which One Is Right for You
For most people with obstructive sleep apnea, CPAP is the effective, sensible, affordable starting point. It is the machine I have relied on for more than a decade, and it changed my life. BiPAP earns its place when CPAP is not the right fit, when exhaling against constant pressure is too hard, when pressures need to run high, or when another breathing condition needs more support than a single pressure can give.
The honest answer to which one is right for you is that your sleep specialist will know better than any article can. What I hope you take from this is enough understanding to ask good questions and to recognize the reasoning behind whatever they recommend. The diagnosis itself, and the road I took from there, is a longer story that I tell in living with sleep apnea if you want to read how this all started for me.
Whichever machine you end up with, the thing that matters most is using it. The best therapy in the world does nothing sitting on the nightstand.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).