Can a Deviated Septum Cause Snoring? Mine Still Did

In my younger days, I had a party trick. I’d grab someone’s cigarette at a party and blow smoke out of one nostril while the other stayed completely sealed. People thought it was some kind of skill. It wasn’t. My septum was so severely deviated that one side was entirely blocked — not partially obstructed, but pressed all the way against the other wall of my nose.
For years, I assumed that was the reason I snored so badly. It made obvious sense: blocked nose, restricted airflow, loud snoring. So when I finally had septoplasty to correct it, I was confident the snoring would stop. I went through the surgery, got through the recovery, waited for the swelling to go down, and waited to discover what sleeping quietly felt like.
My breathing improved dramatically. I could breathe through both nostrils for the first time in my adult life. I went for a run and breathed through my nose the whole way — something I’d genuinely never been able to do. That part felt extraordinary.
But I still snored. Badly. You could hear me from another room, exactly as before.
It took a sleep study some years later to explain why. My AHI was 51. I was stopping breathing more than once a minute, all night, every night. My blood oxygen was dropping to 78 percent. The deviated septum had been a contributing factor, but the actual problem was in my throat — the soft tissue was collapsing repeatedly during sleep and cutting off my airway entirely. No nasal surgery was ever going to fix that.
Why a Deviated Septum Causes Snoring
The mechanism is straightforward. Your nasal septum is supposed to divide your nasal passages into roughly equal halves. When it’s deviated — bent or shifted to one side — one passage becomes significantly narrower, increasing resistance to airflow. Mine was an extreme case, but even moderate deviations create enough restriction to change how you breathe during sleep.
That increased resistance has a few consequences. First, it forces mouth breathing. When the nose can’t move enough air, the body compensates by opening the mouth during sleep. Mouth breathing dramatically worsens snoring because it allows the soft tissues in the throat to vibrate more freely, and it dries out those tissues, making the vibration louder. Second, the effort required to pull air through a restricted nasal passage creates increased negative pressure in the airway — a kind of suction that can make the throat more prone to collapsing. Third, even when nasal breathing is possible, a severely deviated septum creates turbulent airflow that produces its own rattling sound.
All three of these were happening in my case. The septoplasty addressed them. But it was addressing the noise-generating component of a problem whose structural root was elsewhere.
Why Fixing the Nose Didn’t Fix the Snoring
The distinction that most people miss when they’re researching septoplasty for snoring is that snoring can originate in the nose, in the throat, or in both simultaneously — and nasal surgery only addresses one of those locations.
Obstructive sleep apnea is fundamentally a throat problem. During sleep, the muscles that normally keep the upper airway open relax, and in people with OSA they relax far enough that the airway collapses. Each collapse is an apnea event — a complete or near-complete cessation of breathing that lasts until the brain fires enough of an arousal signal to restore airway tone. The snoring associated with sleep apnea is the sound of a partially collapsed airway struggling to pass air. The dangerous part is the complete collapses in between.
A deviated septum makes this picture worse by adding nasal resistance on top of throat obstruction. But correcting the nasal component leaves the throat component entirely intact, which is exactly what I found out the hard way.
A 2024 systematic review published in PMC, covering 25 studies on the role of nasal surgery in obstructive sleep apnea, found that while nasal surgery consistently improves sleep-related quality of life measures, snoring intensity, and daytime sleepiness, it produces no meaningful change in the core polysomnographic measure of OSA severity — the AHI. In other words, patients felt better and snored less loudly, but the underlying apnea events were essentially unchanged. That finding maps precisely to my experience: my nasal breathing transformed, but the deeper problem carried on.
The same review found something worth noting for CPAP users: nasal surgery can meaningfully improve CPAP adherence by reducing nasal resistance and making mask therapy more comfortable. That’s a legitimate reason to consider septoplasty even if you already have an OSA diagnosis — not to fix the apnea, but to make the machine more tolerable.
The Symptoms That Should Prompt a Sleep Study First
The reason I’m so clear that getting a sleep study before pursuing nasal surgery is the right sequence is that the symptoms of sleep apnea and the symptoms of nasal obstruction overlap significantly, and most people can’t tell from the inside which one is driving their problems.
The signs that suggest sleep apnea rather than simple nasal snoring are worth knowing specifically. If a bed partner has witnessed you stop breathing during sleep, even once, that observation warrants a sleep study before anything else. Migraines or consistent morning headaches that improve after you’ve been awake for an hour or two are a classic sign — mine were severe enough to put me in a darkened room vomiting from the pain, and they disappeared within days of starting CPAP. Waking up exhausted despite adequate time in bed, struggling to stay alert during the day, or having near-misses while driving from daytime sleepiness are all red flags that go well beyond what a blocked nose explains.
The American Heart Association’s guidance on sleep apnea and cardiovascular health is worth reading for context on why this matters beyond just feeling tired. Untreated OSA is associated with significantly elevated rates of high blood pressure, stroke, coronary artery disease, and heart failure. I had elevated blood pressure in my early forties that my GP kept noting without either of us connecting it to how I was sleeping. It normalised within months of starting CPAP. The cardiovascular stakes of leaving sleep apnea untreated are not abstract.
Weight loss is another thing I tried before my diagnosis. I lost 20 pounds through sustained exercise and dietary changes. It improved my general health but did nothing to my snoring or my sleep quality, because my apnea was anatomical rather than weight-driven. My AHI was 51, whether I was at my lowest weight or had put a few kilograms back on. That’s a useful data point: if you’ve made significant lifestyle changes and the snoring persists, the problem is likely structural in ways that lifestyle modification alone can’t address.
Getting Diagnosed
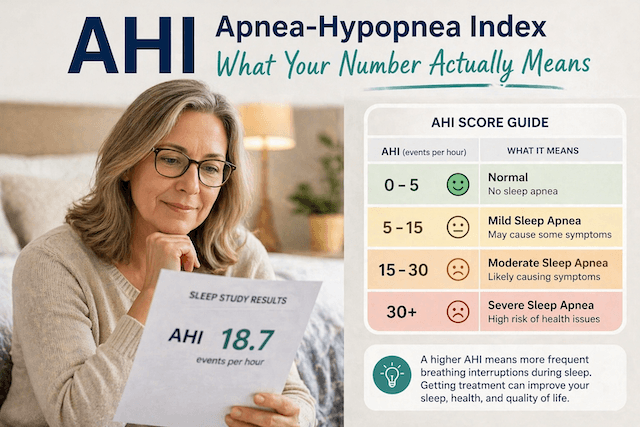
The only way to know whether your snoring involves sleep apnea — and if so how severe — is a sleep study. This produces an Apnea-Hypopnea Index that tells you precisely how many breathing events per hour you’re having and categorises the severity. Under five is normal. Five to fifteen is mild. Fifteen to thirty is moderate. Above thirty is severe. At 51, I was well into the severe category, though I had no idea until the numbers were in front of me.

In-lab polysomnography remains the gold standard, particularly for complex cases. But for most people investigating straightforward suspected OSA, a home sleep test is clinically valid and dramatically more accessible. The WatchPAT One is the one I recommend — it’s FDA-cleared, worn on the wrist for a single night at home, and produces results accurate enough to support a formal diagnosis and treatment plan. If your partner has raised concerns about your breathing, or if you recognise any of the symptoms I’ve described, removing the friction from getting tested is the most useful thing you can do.
What Actually Worked
After my diagnosis, I was prescribed CPAP therapy. I won’t pretend I embraced the idea immediately — the prospect of wearing a mask to sleep for the rest of my life wasn’t appealing. But the results from the first night were striking enough to settle the question quickly. I woke up without a headache. That hadn’t happened in years. The migraines stopped completely and have not returned in over a decade.
My AHI dropped from 51 to around 4-10 overnight and has stayed there consistently since. I use a ResMed AirSense 10 with a full face mask — the full face mask being a deliberate choice given my history of nasal breathing issues. Even after the septoplasty improved my nasal airflow considerably, I prefer the security of a mask that delivers air regardless of whether I’m breathing through my nose or my mouth. For anyone with significant nasal obstruction — whether corrected surgically or not — a full face mask removes nasal breathing as a variable entirely. I’ve written a detailed guide on choosing CPAP masks for deviated septums if you want specific recommendations.
Do I Regret the Septoplasty?
No. The daytime breathing improvements were real and lasting. I can exercise without gasping. My sinus drainage improved. The quality of life difference from being able to breathe through my nose properly was significant, and I don’t regret having the surgery. I just regret having expected it to solve a problem it wasn’t designed to solve.
The version of me that went into that surgery had never been told that snoring and sleep apnea are different things with different causes and different treatments. I assumed fixing the most obvious structural abnormality in my airway would fix everything upstream of it. That assumption cost me years of undiagnosed severe OSA.
If I could go back and give myself one piece of advice, it would be this: get the sleep study first. Before considering any surgery for snoring, before assuming you know what’s causing the problem, get the data. If the study rules out significant OSA, you can pursue nasal surgery with a clear picture of what it can and can’t achieve. If it confirms OSA, you know the priority is treating the airway, not the nose, and any nasal surgery you do subsequently becomes an adjunct to that treatment rather than a substitute for it.
The smart order of operations is diagnosis first, then decisions. Don’t make the mistake I made of assuming fixing one thing will fix everything.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).