How does ASV work? Exploring the Science Behind the Machine

I use CPAP. I’ve used it for over eleven years and it manages my obstructive sleep apnea well. But over the years of running this blog I’ve spoken to and heard from a lot of people for whom CPAP isn’t the right answer, either because their sleep apnea has a central component, or because treatment-emergent central apneas developed after they started CPAP, or because they have a condition like heart failure that produces Cheyne-Stokes breathing patterns that standard PAP therapy can’t address properly.
For those people, the next step is often Adaptive Servo-Ventilation, or ASV. And the most common question I see from people who’ve been told they need it is: what exactly does it do that CPAP doesn’t?
The answer is genuinely interesting and worth understanding properly, because the difference isn’t just a matter of degree. ASV does something fundamentally different from either CPAP or BiPAP, and understanding why explains both why it works for conditions those devices can’t manage and why it isn’t simply a better version of CPAP that everyone should want.
What CPAP and BiPAP Actually Do
To understand what makes ASV different, it helps to be clear on what the other devices do.
A CPAP machine delivers a single fixed pressure continuously throughout the night. That constant positive pressure acts as a pneumatic splint for the airway, preventing the soft tissue from collapsing. It works well for obstructive sleep apnea because obstructive apneas are caused by physical collapse of the airway, and a constant pressure stops that collapse from happening.
A BiPAP machine delivers two pressures: a higher one during inhalation and a lower one during exhalation. This makes it easier for people who find exhaling against high pressure uncomfortable, and it provides some ventilatory support that a fixed-pressure CPAP doesn’t. But both CPAP and BiPAP operate on a fundamentally static model: they deliver the same pressures regardless of what your breathing is doing moment to moment.
That works fine when the problem is mechanical obstruction. It doesn’t work for breathing disorders where the problem is in the brain’s respiratory control rather than the airway itself.
The Problem ASV Is Designed to Solve
Central sleep apnea is different from obstructive sleep apnea in an important way. The airway isn’t collapsing. The breathing stops because the brain isn’t sending the right signals to the respiratory muscles. There’s nothing for a fixed pressure to splint because there’s no obstruction to prevent.
Complex sleep apnea involves both obstructive and central components, and presents a particular challenge because sometimes central apneas emerge or worsen when obstructive apneas are treated with CPAP. The CPAP resolves the obstruction, but the central breathing instability remains or becomes more apparent.
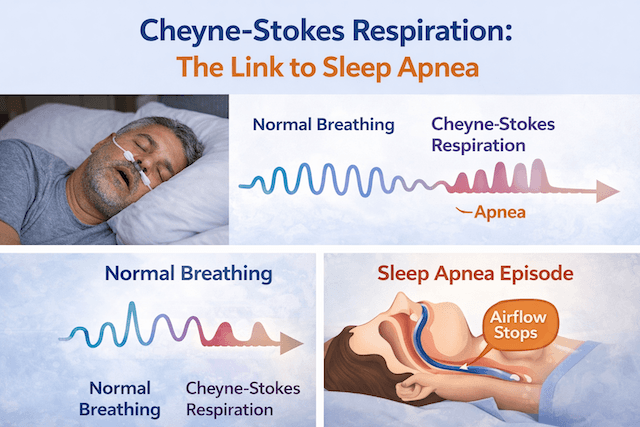
Cheyne-Stokes respiration, which is associated with heart failure, produces a distinctive cyclical breathing pattern where breathing gradually increases, then decreases, then pauses, then starts again. It’s a sign that the brain’s respiratory feedback loop is dysregulated, and it can’t be addressed by holding the airway open with constant pressure.
What all of these conditions share is variable, unpredictable breathing that needs something more sophisticated than a constant or two-setting pressure device. They need a machine that responds to what’s actually happening on each individual breath.
What the Adaptive in ASV Actually Means
The word adaptive is doing real work in the name. An ASV machine doesn’t deliver a predetermined pressure. It continuously monitors your breathing and calculates a target ventilation level based on your recent breathing history, typically a rolling average of the past few minutes. It then delivers exactly as much pressure support as is needed on each individual breath to keep your actual ventilation close to that target.
If your breathing becomes shallow or pauses, the machine increases inspiratory pressure support to compensate. If you’re breathing adequately on your own, it reduces support to the minimum needed to maintain airway patency without over-ventilating you. If you’re breathing excessively, it backs off further. The adjustment happens breath by breath, in real time, with changes occurring in milliseconds.
The machine maintains a baseline expiratory pressure to keep the airway open, which handles any obstructive component. On top of that it adds variable inspiratory support that responds dynamically to your respiratory effort. The two together address both the mechanical airway obstruction and the central breathing instability simultaneously.
This breath-by-breath responsiveness is what CPAP and BiPAP cannot do. CPAP holds a fixed pressure and waits for you to breathe. BiPAP cycles between two fixed pressures. ASV watches each breath, predicts what the next one needs, and delivers it.
Why This Matters for Central Apneas Specifically
There’s a concept in respiratory physiology called loop gain, which describes how sensitive the body’s breathing control system is to changes in carbon dioxide levels. High loop gain means small fluctuations in CO2 produce large overcorrections in breathing rate, which leads to the oscillating pattern of over-breathing and under-breathing that characterises central sleep apnea and Cheyne-Stokes respiration.
ASV stabilises this feedback loop by taking over the moment-to-moment ventilation regulation that the brain is struggling to perform consistently. By smoothing out the CO2 fluctuations that drive the instability, it breaks the cycle rather than just responding to each individual apnea event after it occurs. This is why it works where BiPAP’s fixed pressure support doesn’t: BiPAP provides consistent support regardless of what the breathing is doing, which can actually amplify the instability rather than dampen it.
How It Compares in Practice
For someone with straightforward obstructive sleep apnea like mine, ASV offers no advantage over a well-titrated CPAP or APAP. The breathing instability that ASV addresses isn’t present. Adding variable pressure support to a system that just needs its airway held open adds complexity without benefit.
For someone with central or complex sleep apnea, or Cheyne-Stokes respiration from heart failure, ASV is typically dramatically more effective than anything else currently available. Studies have shown that ASV reduces the apnea-hypopnea index to near-normal levels in central sleep apnea patients where CPAP had made little difference, with corresponding improvements in sleep quality, daytime functioning and cardiovascular markers in appropriate patient groups.
The important caveat, which I’ve covered in more detail in my ASV applications article, is that ASV is contraindicated in heart failure patients with reduced ejection fraction following the SERVE-HF trial findings. If heart failure is involved, the ejection fraction needs to be properly assessed before ASV is prescribed. This is a clinical decision that belongs with a cardiologist and sleep specialist, not something to navigate independently.
What It’s Like to Use
In practical terms, an ASV machine looks and feels similar to a BiPAP from the user’s perspective. It uses the same types of masks, the same basic setup process, and connects to similar data tracking apps. The ResMed AirCurve 10 ASV is the most commonly prescribed device in this category, and most people who’ve struggled with central apneas on CPAP describe the adjustment to ASV as straightforward.
The noticeable difference is in the breathing experience. Rather than breathing against a constant pressure or cycling between two fixed levels, the machine feels more natural to breathe with because it’s responding to what you’re doing rather than imposing a fixed rhythm. People who’ve experienced treatment-emergent central apneas on CPAP, where adding pressure was making the central events worse, often describe ASV as the first therapy that let them actually sleep.
Who Needs to Be Asking About This
If you’re currently on CPAP and your therapy data is showing persistent central apnea events despite good compliance and well-controlled obstructive events, it’s worth raising with your sleep clinic. Treatment-emergent central apneas affect a proportion of CPAP users and often go undiscussed because the overall numbers can look acceptable while the central component remains.
If you have heart failure and are experiencing sleep-disordered breathing, the question of whether it’s primarily obstructive or central matters enormously for treatment choice, and that distinction requires a proper sleep study and cardiology input rather than assumption.
And if you’ve been told your CPAP isn’t adequately controlling your sleep apnea despite good compliance and appropriate settings, asking whether the problem might have a central component is a reasonable next question to put to your specialist.
ASV isn’t the answer for most people with sleep apnea. CPAP does the job well for the majority. But for the people who need it, it does something that nothing else currently can, and understanding why is useful whether you’re a patient trying to make sense of a recommendation or simply curious about how the technology works.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).