How I’ve Stayed Consistent With CPAP Therapy

The CPAP machine sitting on your nightstand only works if you actually wear it. I have been on therapy for more than a decade, and the honest answer to “how did you stay consistent” is unglamorous. I built a small daily routine that does not require willpower, and I dealt with problems early so they never became reasons to quit.
If you are new to CPAP, or if you have been prescribed a machine and it has been gathering dust, this post is for you. I am not a doctor. My background is in computer science. But I do have years of personal experience sticking with this therapy through travel, illness, camping trips, and the ordinary grind of weekday life, and I want to share what has actually worked.
The numbers most people are not told
A fact most people do not realize when they receive their machine is that the research on CPAP adherence is genuinely sobering. A widely cited review by Weaver and Grunstein in Proceedings of the American Thoracic Society found that, depending on how compliance is defined, 46 to 83 percent of patients with obstructive sleep apnea are nonadherent to treatment. That is not a fringe finding. It is the central problem of the therapy.
Insurance providers, including Medicare in the United States, generally use what is called the four hour rule for CPAP compliance: at least four hours of use per night on at least 70 percent of nights inside a 30 day window. The Sleep Foundation has a good primer on what that actually looks like in practice. The four hour threshold exists because it is the floor at which insurers will keep paying for your equipment, not because it is the level at which you get the most benefit.
The same body of research suggests the real gains in daytime alertness, memory, and reduced cardiovascular strain show up at six hours or more of nightly use. So the four hour rule is the floor for keeping your equipment subsidized. Consistency above that is what gives you back your life.
When I was starting out, I had nights where I clocked four hours and thought, good enough. The honest reframe for me was understanding that I was treating a serious medical condition, not hitting a quota.
Why most people quit, and what to do instead
The same adherence research has a second finding that is even more useful. The pattern of CPAP use is established in the first week of treatment, and it predicts whether you will still be using your machine a year from now. People who push through the early discomfort tend to stick with therapy. People who do not tend to quit within weeks.
Here is what I think most patients miss. People rarely quit CPAP because they decide CPAP does not work. They quit because of a fixable problem they tried to live with. The mask leaks. The pressure feels wrong. The hose drips condensation onto their face. The straps leave marks. None of these is a reason to abandon a serious medical therapy. All of them are problems your provider can solve, often in a single appointment. Mayo Clinic has a useful overview of the most common CPAP problems and how to address them, and it lines up almost exactly with the issues I have heard from other CPAP users over the years.
When I was diagnosed with severe obstructive sleep apnea, my AHI was 51, which means I was averaging roughly 51 breathing events every hour I slept. The first nights with the mask were strange. I will not pretend they felt natural. The pressure was unfamiliar, the headgear felt awkward, and there was the basic absurdity of strapping a piece of medical equipment to your face before bed.
What helped me get past the first month was treating it as a settling in period rather than a test I might fail. I gave myself permission to take the mask off if I genuinely could not sleep, but I put it back on as soon as I could. I used the ramp feature on my ResMed AirSense 10, which starts air pressure low and gradually increases as you fall asleep. And I called my equipment supplier when something did not feel right, rather than waiting it out.
If you are reading this on your first night with CPAP right now, the most important advice I can give you is to be a squeaky wheel. Mask uncomfortable? Pressure feels off? Air leaking out the side? Do not tough it out for weeks. Call your provider. Most early problems are fixable, and people who quit therapy almost always quit because of a problem that could have been fixed.
The mask is the single biggest factor
If your mask is wrong for your face or your sleep style, no amount of motivation will save you. If it is right, you stop thinking about it.
I am a chronic mouth breather, which is its own subspecies of CPAP user. With a nasal mask or nasal pillows, I would open my mouth in my sleep and the pressurized air would simply escape. So I have used a full face mask throughout my therapy. If you also breathe through your mouth at night, masks designed for mouth breathers are worth looking at first rather than working through the other categories one at a time.
Mask fit is also not a one and done decision. Cushions wear out. Faces change. If your seal has been getting worse over weeks, replace the cushion before you replace the mask. If it is still not working, ask your supplier about trying a different size or a different model. Most suppliers will let you swap inside the first 30 days. The troubleshooting CPAP problems and why does my CPAP mask leak posts cover diagnosing what is actually going wrong before you give up on a setup.
A small daily routine that does not need willpower
The mask going on at bedtime is now as automatic for me as brushing my teeth, but it did not get there by accident. The rhythm built itself over time around two simple habits.
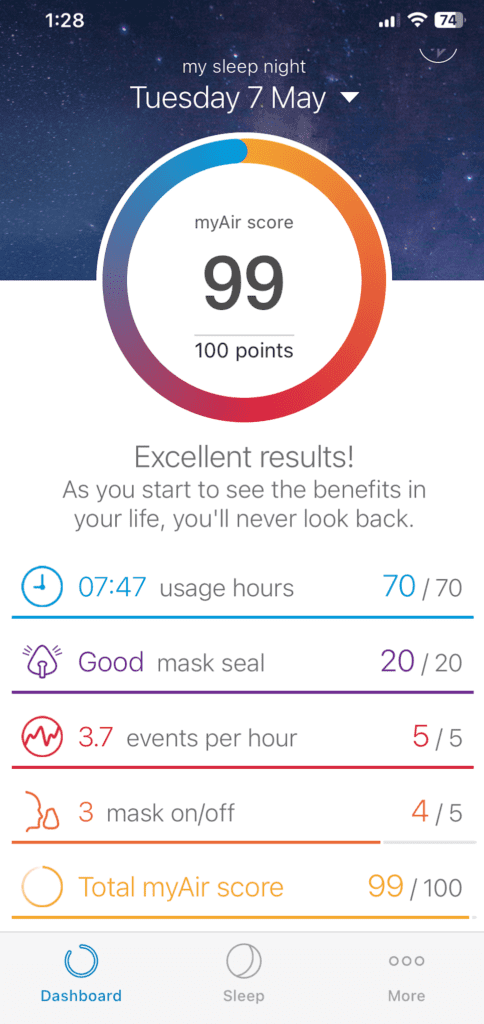
In the morning, I check the ResMed myAir app on my phone. The AirSense 10 syncs my night’s data wirelessly, and myAir shows me my usage hours, my mask seal quality, and my events per hour. I am not obsessive about the score. What I am looking for is whether something has changed. If events per hour ticked up or my mask leaks went sideways, that tells me something needs attention before it turns into a week of bad sleep. The morning glance takes seconds and saves me a lot of trouble.
Then I clean the mask cushion. This is the only part of the routine I treat as nonnegotiable. Facial oils and dead skin cells build up on the silicone overnight, and that buildup is the single biggest reason mask seals deteriorate. A rinse with warm water and a little mild soap, followed by air drying, is enough. The cushion is dry by bedtime and the seal stays good for far longer than it does when I get lazy about this step.

Once a week, I do a deeper clean: hand-wash the headgear and straps, run warm soapy water through the hose, soak the humidifier chamber, and check the filter. The full step by step is in my how to clean a CPAP machine post if you want it.
A couple of things I have learned about cleaning. First, distilled water in the humidifier really does matter. Tap water leaves mineral deposits that shorten the life of the chamber. Second, dirty equipment does not just smell bad. It leaks. A worn or oily cushion stops sealing, and a leaking mask is the most common reason people abandon therapy. Cleaning is not just hygiene. It is consistency insurance.

Travel is where most people fall off
CPAP therapy has one obvious enemy, and it is travel. The full machine, the hose, the humidifier chamber, and a jug of distilled water are not what you want to drag through an airport or pack into a tent.
My answer was to invest in a ResMed AirMini for travel and camping. It is small enough to pack into hand luggage, and it has gotten me through international trips and camping nights without missing therapy. If you have been skipping CPAP on holidays or work trips, a travel machine is the most practical investment you can make in your own consistency. My posts on traveling with CPAP and camping with a CPAP machine cover the practical details.
What I will not do, and what I would push back on if anyone suggested it, is treat a night without CPAP as harmless. The same adherence research notes that even one skipped night allows daytime sleepiness and other deficits to reemerge. If you cannot bring the machine somewhere, the question is really whether the trip is worth that cost.
The mental side, or remembering why you started
There are still nights, even now, where putting the mask on feels like a hassle. What gets me past it is a short, honest conversation with myself about what untreated sleep apnea actually does.
I have written separately about my diagnosis story, but the short version is that without my wife pushing the issue I might not have been diagnosed at all. Severe untreated OSA carries real, well documented cardiovascular consequences and stroke risk. CPAP did not cure my sleep apnea. It treats it, every night, on the nights I use it. Skipping is a choice to undo the treatment.
That framing has done more for my consistency than any app score. The mask is not a punishment. It is the thing keeping me on the safe side of a serious chronic condition.
If you are feeling resistance to therapy, particularly anxiety or claustrophobia around the mask, I would encourage you to take it seriously rather than push through. Anxiety is a real reason people quit, and there are real strategies for it. Avoiding the issue tends to make it harder, not easier. A conversation with your sleep doctor, or in some cases with a counselor, is worth more than another month of trying to power through.
A few things I would tell someone starting out
The first two weeks are the hardest. They are not representative of how the rest of your therapy will feel. By the third month, the mask should feel normal, and by the sixth month, you should be sleeping better than you have in years. If that is not happening, something in your setup needs adjusting, and the conversation to have is with your sleep doctor or your equipment provider.
Consumables wear out, and replacing them on schedule is part of staying consistent. Mask cushions every month or two, headgear every six months or so, hoses every few months. The full CPAP replacement schedule is on the site. I have watched people blame themselves for poor therapy when the real problem was a six month old cushion that had quietly lost its seal.
Do not suffer in silence. If you are getting dry mouth, aerophagia, rainout in the hose, or skin irritation, those are all common and all fixable. Most are a fifteen minute conversation with your provider. None of them is a reason to give up on therapy.
Watch your data, but do not worship it. My morning myAir glance is a tool for catching problems early, not a scoreboard to feel good or bad about myself. If you find yourself stressing over your score the way some people stress over their step count, you have made the metric the goal. The goal is sleep, and a body that wakes up rested.
The honest summary
CPAP is a chronic disease therapy, not a temporary fix. After more than a decade on it, what I can tell you is that the daily reality is far less dramatic than it sounds. A mask goes on at night. It comes off in the morning. The cushion gets washed. Every so often something breaks or wears out and gets replaced. The rest is just sleeping.
If you can build that rhythm and stick with it, the therapy does its job. And after long enough, you stop thinking of yourself as someone with sleep apnea who has to use CPAP, and start thinking of yourself as someone who sleeps well, with a small piece of equipment that makes that possible.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).





