Sleep Apnea and Atrial Fibrillation: What CPAP User Should Know

I want to be straight with you before this article goes any further. I have severe obstructive sleep apnea, and I have used CPAP for more than a decade. I have a computer science background, not a medical one. And I have not been diagnosed with atrial fibrillation. What follows is a careful look at a connection that comes up constantly in the sleep apnea community, written by a patient who has spent years reading the research and talking to other patients, but who is not in a position to give medical advice.
That disclosure matters because the link between sleep apnea and atrial fibrillation, usually shortened to AFib, is one of the most consequential things a long term CPAP user can understand. The two conditions sit so close to each other in the cardiology and sleep medicine literature that major heart organizations now recommend screening for sleep apnea in people with recurrent AFib. If you have sleep apnea, or you suspect you do, the AFib question is worth your attention.
What atrial fibrillation actually is
Atrial fibrillation is the most common sustained abnormal heart rhythm in adults. In a normal heartbeat, the upper chambers of the heart, the atria, contract in a coordinated way that pushes blood into the lower chambers, the ventricles, which then pump it out to the lungs and the body. In AFib, the electrical signals in the atria become chaotic. Instead of a steady, organized contraction, the atria quiver. The ventricles still beat, but they do so irregularly and often too fast, because they are responding to a disorganized signal from above.
Some people feel AFib as a fluttering, pounding, or skipping in the chest. Some feel short of breath, lightheaded, or unusually tired. Others feel nothing at all and discover the arrhythmia only when a doctor picks it up on a pulse check or an ECG. AFib can be paroxysmal, meaning it comes and goes on its own, or persistent, meaning it stays unless something is done to restore the normal rhythm.
The reason AFib matters so much is that quivering atria allow blood to pool, which raises the risk of clots forming and traveling. That is why stroke risk is one of the central concerns in AFib management, and why a lot of treatment is aimed at preventing clots in addition to controlling the rhythm itself.
The documented link with sleep apnea
The connection between obstructive sleep apnea and atrial fibrillation is not a fringe theory. The American Heart Association has published a scientific statement noting that obstructive sleep apnea is highly prevalent in people with atrial fibrillation, with prevalence figures in cardiac populations running far higher than in the general adult population. The AHA describes sleep apnea as common in people with hypertension, heart failure, coronary artery disease, pulmonary hypertension, atrial fibrillation, and stroke, and specifically recommends screening for sleep apnea in patients with recurrent AFib after cardioversion or ablation procedures. You can read the AHA’s plain language overview of the heart and sleep apnea connection on their Sleep Apnea and Heart Health page.
The Sleep Foundation, summarizing the same body of research for a general audience, frames the relationship in similar terms. People with sleep apnea are estimated to be two to four times more likely to develop heart arrhythmias than people without it, and the mechanisms include intrathoracic pressure changes, oxygen swings, and chronic sympathetic nervous system activation. Their overview is at Sleep Apnea and Heart Disease if you want to read it in full.
What these statements are not saying is that everyone with sleep apnea will develop AFib. They are saying that the two conditions cluster together far more than chance would predict, that there are plausible biological reasons why one promotes the other, and that anyone with AFib should at least be evaluated for an underlying sleep breathing problem. For the patient population I write for, the implication runs the other way as well. If you have moderate to severe sleep apnea and you are not using your therapy consistently, you may be sitting on top of one of the strongest modifiable risk factors for AFib that medicine has identified.
Why the biology makes sense
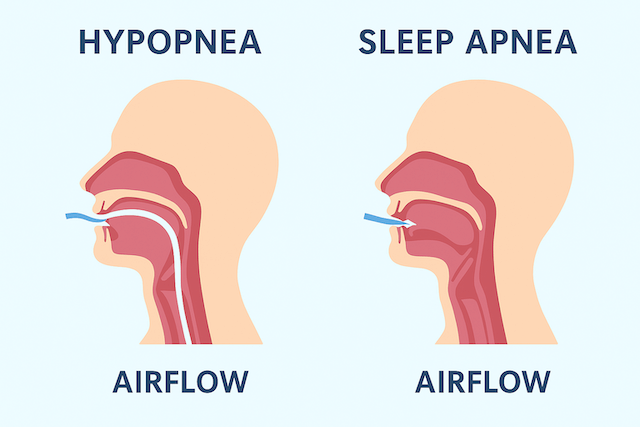
The biological pathway from sleep apnea to atrial fibrillation is one of the more intuitive parts of all this once you understand what an apnea event is doing to the body. I have written elsewhere about how obstructive sleep apnea works mechanically, but the short version is that the upper airway collapses during sleep, you keep trying to breathe against a closed pipe, and the body experiences a series of stresses that nothing about normal sleep is designed to handle.
Three of those stresses are particularly relevant to the heart.
The first is the swing in intrathoracic pressure. When you try to inhale against a closed airway, you generate strongly negative pressure inside the chest. The heart sits inside that chest cavity, and over time these repeated pressure changes pull on the atria and stretch the tissue. Stretched atria are more electrically irritable. They become a more hospitable environment for the disorganized signals that drive AFib.
The second is the repeated drop in blood oxygen. During an apnea event, oxygen saturation falls. The body interprets this as an emergency, releases a surge of stress hormones, and pushes the heart to work harder. If this happens once in a blue moon, the heart absorbs it without complaint. If it happens dozens of times an hour, every night, for years, the cardiovascular system pays a price. I have a longer piece on blood oxygen levels during sleep for readers who want to dig into the oxygen side of this.
The third is the activation of the sympathetic nervous system. Apnea events trigger arousals, sometimes conscious but usually not, and these arousals come with bursts of adrenaline and noradrenaline that raise blood pressure and accelerate the heart. Over time this chronic sympathetic activation contributes to hypertension, vascular damage, and the kind of background electrical instability that can tip a vulnerable heart into AFib.
None of these mechanisms is hypothetical. They are measurable, and they are present every night that an untreated apneic patient sleeps. The size of the AHI score gives you some sense of how many of these events are happening per hour. My AHI at diagnosis was 51, which means severe sleep apnea. I have thought a lot about what those numbers were doing to my heart in the years before I started therapy.
AFib while sleeping: why people search for this
A lot of people land on articles about sleep apnea and AFib because they have noticed their heart doing strange things at night. They wake up with a pounding chest. They feel their pulse race for no reason. They notice an irregular flutter as they are drifting off. They search “AFib while sleeping” or “heart palpitations at night” and end up reading about sleep apnea.
There are a few things going on here. AFib does have a tendency to start at night in many patients, and sleep apnea is one of the reasons why. The vagal tone shifts that happen during sleep, combined with the apnea induced stresses described above, can act as a trigger. Some people have a pattern where their AFib episodes cluster in the early morning hours, which is also when REM sleep is most concentrated and when obstructive events tend to be worst.
But it is also worth saying that not every nocturnal heart palpitation is AFib. The sensation of the heart racing or pounding at night can come from anxiety, from acid reflux, from caffeine still circulating, from a fever, from premature ventricular contractions which are mostly benign, and from a number of other causes that have nothing to do with sleep apnea. The honest answer to “can sleep apnea cause heart palpitations” is yes, it can, but it is not the only thing that can, and the only way to know whether what you are feeling is AFib or something else is to capture it on an ECG.
If you have a wearable that does single lead ECGs, that capability has become quite useful for situations like this. If you do not, and you are getting persistent or frightening nocturnal palpitations, that is a conversation to have with your doctor sooner rather than later.
Does treating sleep apnea help AFib?
This is the question that matters most for CPAP users, and the answer the research supports is a qualified yes, with some caveats worth understanding.
Multiple studies have looked at patients who underwent procedures to restore normal heart rhythm, either electrical cardioversion or catheter ablation, and tracked whether their AFib came back. The pattern that has emerged repeatedly is that patients with untreated sleep apnea have substantially higher AFib recurrence rates than patients without sleep apnea, and that patients who use CPAP consistently have recurrence rates closer to the non apneic group. This is why cardiology guidelines now suggest evaluating recurrent AFib patients for sleep apnea. The therapy is not a cure, but it appears to remove one of the engines that keeps pushing the heart back into the arrhythmia.
The caveat is that the evidence for CPAP preventing AFib in the first place, in someone who has sleep apnea but has never had an AFib episode, is less settled. Some large randomized trials have not shown the dramatic cardiovascular benefit that observational studies suggested. There are a few likely reasons for this. People assigned to CPAP in trials often do not use it for enough hours per night to get the full effect. The patients selected for trials are sometimes a milder slice of the apneic population than the cardiac patients who actually drive the AFib link. And cardiovascular outcomes take many years to play out, which makes them hard to capture in trial timeframes.
What you can say with confidence is that consistent CPAP use addresses the mechanisms that drive AFib in apneic patients, that the cardiology field considers it part of standard AFib management when sleep apnea is present, and that the patients with the best outcomes are the ones who treat their apnea seriously rather than half-heartedly. If you want to see the broader picture of why this matters for the heart, my page on sleep apnea and cardiovascular health covers more of the territory.
A separate note on central sleep apnea and AFib
Most of the discussion above is about obstructive sleep apnea, which is what I have and what the majority of readers of this site have. There is a separate connection between central sleep apnea and AFib, and it deserves a brief mention because the treatment picture is different and more delicate.
Central sleep apnea, in contrast to the obstructive variety, is a problem with the brain’s signal to breathe rather than a mechanical airway collapse. It is much less common than OSA but shows up more often in patients with heart failure and in some patients with AFib. The relationship in this group can be complex. One trial of adaptive servo ventilation, a more sophisticated form of positive airway pressure therapy, in heart failure patients with central sleep apnea found that the therapy actually increased cardiovascular mortality, which was the opposite of what researchers expected. That is not a finding that applies to obstructive sleep apnea treated with standard CPAP, but it is a reminder that the heart and the breathing control system interact in ways that are still being worked out. If you have AFib and your sleep study turns up central rather than obstructive events, you want a sleep specialist and a cardiologist working together on your treatment plan, not a generic prescription.
Signs your sleep apnea might be affecting your heart
There is no symptom that proves your sleep apnea is causing AFib, but there are patterns that make the cardiac story more likely. Loud snoring with witnessed pauses in breathing is the classic OSA presentation, and if a partner has watched you stop breathing during sleep, that observation carries real weight. Waking up with a pounding or racing heart, especially in the early morning, is another signal worth paying attention to. Morning headaches, daytime fatigue that does not improve with more sleep, nocturia (which I have written about separately because the mechanism connects to the same hormonal cascade that strains the heart), and resistant high blood pressure that does not respond well to medication all belong on the same list.
The other red flag is being told by a cardiologist that your AFib has been hard to control. Recurrent AFib after cardioversion or ablation, AFib in someone who does not fit the usual risk profile, and AFib that gets worse rather than better despite treatment are all situations where sleep apnea is worth ruling out. This is exactly the scenario the AHA scientific statement is talking about when it recommends screening.
What I have done with this information personally
I cannot tell you what to do about your heart. I can tell you what this body of research has done to my own behavior as a long term CPAP user.
It has made me serious about compliance. I do not skip nights. I travel with my ResMed AirMini so that camping trips and international travel do not turn into untreated apnea stretches. I keep an eye on my mask seal because a leaking mask is a half treated night. I have written elsewhere about CPAP compliance and about why I am suspicious of the framing that CPAP is somehow optional once you start feeling better. The reason it matters is exactly this: the mechanisms that drive AFib do not switch off because you have stopped feeling sleepy. They keep working in the background as long as the apnea is untreated.
It has also made me pay closer attention to the rest of the cardiovascular picture. Blood pressure, weight, alcohol intake, exercise. None of that is unique to apnea patients, but the AFib evidence sharpens the stakes. If you are someone with severe sleep apnea and you are doing one part of cardiovascular care well and the other parts not at all, you are leaving a lot on the table.
And it has made me unwilling to put off the AirSense 11 upgrade conversation forever. I have been using two AirSense 10 machines for the better part of a decade and they have served me well, but the therapy data and the comfort improvements on newer machines are real, and there is no prize for clinging to old hardware when better tools exist. If you want to read more about the current generation, my ResMed AirSense 11 review covers what I have learned from the research and from other users.
Where to take this from here
If you have AFib and have never been evaluated for sleep apnea, that conversation with your cardiologist is worth having. The current cardiology guidelines support it. If you have sleep apnea and you have ever felt your heart doing strange things at night, do not write it off, especially if you are not consistent with your therapy. And if you are reading this because you suspect you might have either condition, the first step is getting tested rather than self diagnosing from articles like this one. The pieces I have written on living with sleep apnea and on overcoming the early CPAP anxiety might be useful if it turns out you are about to start therapy.
The thread that runs through all of this is the same thread that runs through most of what I write. Sleep apnea is not just a sleep problem. It is a whole body condition that has been linked, in serious peer-reviewed research, to consequences in the heart, the brain, the metabolism, and the lifespan. AFib is one of the clearest examples of why the therapy is worth taking seriously even on the nights you do not feel like putting the mask on.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).