How to Overcome CPAP Anxiety: What Actually Helps
I’ll be upfront about something first.
Severe CPAP anxiety isn’t something I personally struggled with when I started therapy more than a decade ago. The headaches and migraines I’d been waking up with had become so debilitating that the relief CPAP brought outweighed every discomfort the equipment gave me. Yes, the mask felt like an alien strapped to my face the first few nights. But after years of waking up with my head pounding, that was a trade I was happy to make.
That’s my story. I know it isn’t everyone’s. Spend any time in CPAP Facebook groups or on r/SleepApnea and you see the same posts come up week after week. People who can’t stop pulling the mask off in their sleep. People who’ve had panic attacks the moment the airflow starts. People whose machines are sitting unused in a closet because they couldn’t get through the first night.
CPAP anxiety is one of the most common reasons people quit therapy before it has a chance to help them. So this page isn’t me telling you how I beat CPAP anxiety. It’s what the research says about why CPAP anxiety happens, what people in the sleep apnea community consistently say has helped them work through it, and the parts of my own experience that genuinely apply.
A note before we go further. I’m not a doctor. My background is in computer science. Everything below is general information drawn from published research and from a long time spent reading and listening to people who use these machines. It is not medical advice. If CPAP anxiety is making it impossible for you to use your machine, talk to your sleep clinic. They have options I can’t prescribe.
Why CPAP Anxiety Is So Common
A 2015 study published in the journal Heart & Lung looked at adults newly starting CPAP and found that 63% had what the researchers called “claustrophobic tendencies” after their first night with the mask on. The same study found women experienced this more often than men, and that those tendencies were strongly linked to people not sticking with therapy in their first month.
Sixty three percent. That isn’t a fringe problem. If you’re in that group, you’re not unusual, and you’re definitely not weak. You’re having one of the most well documented reactions to CPAP that exists.
The same paper described claustrophobia as having two parts: fear of restriction and fear of suffocation. Both kick in the moment a mask seals to your face. Your nervous system reads the situation as something covering me and changing how I breathe, and it doesn’t always wait for your conscious brain to catch up and say this is fine, this is therapy.
The cruel irony is that the people who need CPAP most are often the ones whose nervous systems are most primed to react this way. If you have severe sleep apnea, you’ve spent years with your body waking itself up dozens of times a night because it thinks it’s suffocating. Your stress response is well rehearsed. Asking it to stay calm while a mask seals to your face is asking a lot of it.
What the Mask Actually Does (And Why It’s Safe)
Modern CPAP masks have safety vents built into them. They have to. Air comes in from the machine, but carbon dioxide needs a way out, and the mask is designed so that even if the machine were to stop running, you’d still be able to breathe room air through the vents. You cannot suffocate inside a properly fitted CPAP mask. The mask isn’t sealing you in. It’s just delivering pressurized air with a clear path back out.
That’s true. It’s also useless information when your body is in fight or flight mode at bedtime and your brain is telling you to rip the thing off.
What people in the CPAP community keep saying, and what behavioral health research backs up, is that you can’t logic your way past this in the moment. The fear isn’t a thinking problem. It’s a feeling problem. The path through is letting your nervous system learn, slowly, that the mask is safe. Not by reading about safety vents. By spending time with the equipment until your body files it under neutral instead of threat.
What People Find Actually Helps
The strongest pattern across community forums and the behavioral research is the same one a sleep specialist would tell you. Don’t try to wear the mask for a full night on day one if it scares you. Build up to it.
Hold the mask up to your face for a few seconds while sitting on the couch. Watch TV. Put it down. Pick it up again. Do this until holding it feels like nothing.
Then put the straps on, machine off. Get used to the feel of headgear. Take it off whenever you want to.
Then turn the machine on while you’re sitting up, awake, doing something low pressure. The airflow will feel strange. That’s expected. The first time it stops feeling strange might be the tenth time, not the second.
Then try a daytime nap with the full setup. Then try bedtime, knowing that if you take it off after twenty minutes, that’s still twenty minutes of progress.
This is what behavioral therapists call graded exposure or systematic desensitization. A randomized trial published in the journal Sleep found that patients who received structured behavioral coaching used their CPAP roughly twice as many hours per night as those who got standard care. The technique is unglamorous, and it works.
What community posts agree on, almost unanimously, is that doing any of this is better than doing none of it. People who push through one panicked first night often have a worse second night, because their nervous system has now logged mask equals panic. People who back up and do the boring couch time first usually get there faster in the end.
Pace matters more than progress. If you’ve practiced with the mask off for three days and that still feels like enough, stay there for a fourth. If turning the machine on for ten minutes is your ceiling this week, that’s the ceiling. Push when it feels manageable. Don’t push when it doesn’t.
The Mask Itself Matters More Than People Think
A lot of what gets called CPAP anxiety isn’t really anxiety. It’s a poorly fitting mask that’s leaking, blowing air into your eyes, or pressing on a nerve, and your body is rightly upset about it.
I’m a chronic mouth breather, so I’ve only ever used a full face mask. The current one is a ResMed AirFit F20. I went straight to full face on my sleep clinic’s recommendation and never trialed nasal pillows or nasal masks myself, so I can’t give you a personal comparison there. What I can tell you is that getting the fit right made the whole thing easier. A mask that’s pulling on your skin or whistling air into the corner of your eye every time you turn your head will make anyone anxious, fast.
If you’re a mouth breather and you’ve been issued a nasal mask or nasal pillows, that mismatch alone can drive most of what feels like anxiety. The community consensus, and my own clinic’s recommendation, is that the wrong mask type is one of the biggest fixable causes of early therapy struggle. If you suspect this is what’s happening to you, talk to your equipment supplier about a different style. There’s a guide to the best CPAP masks for mouth breathers on the site if you want to read about specific options.
A few other equipment factors that come up in community discussions over and over:
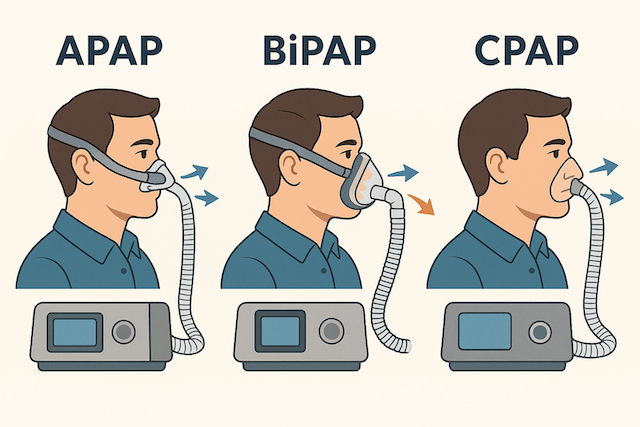
The ramp feature, on most modern machines, starts the pressure low and increases it gradually as you fall asleep. If your prescribed pressure feels overwhelming the moment you put the mask on, ramp can soften the entry point. It’s usually adjustable from your machine’s menu.
Expiratory pressure relief, called EPR on ResMed machines, drops the pressure slightly when you exhale so it feels less like fighting the airflow. Not every machine has it set to active by default. If breathing out against the pressure is what’s bothering you, ask your clinic whether EPR is enabled and at what level.
Humidification, especially in dry climates, prevents the kind of nasal irritation and dry mouth that wakes people up feeling like something is wrong. Most current machines have a built in humidifier with adjustable settings. There’s more on the basics here: CPAP humidifier guide.
If your prescribed pressure is wrong for you, the whole night feels like a struggle. This is not something to adjust on your own, but it is something to bring up with your sleep clinic if you’re consistently uncomfortable. Pressure that’s too high for your needs can produce a feeling indistinguishable from anxiety. So can pressure that’s too low, because the underlying apnea events keep happening and your body keeps trying to wake you up.
Breathing Techniques People Mention
I don’t personally use breathing exercises before bed. The migraines were so insistent on me using the machine that the mask never had time to become a battle. But breathing exercises come up often enough in the community that they’re worth mentioning, because for many people they help.
The one most frequently recommended is 4-7-8 breathing, where you inhale through your nose for a count of four, hold for seven, and exhale through your mouth for eight. The Cleveland Clinic has a write up on it as a relaxation technique. The reason this kind of slow, paced breathing gets recommended for CPAP anxiety is that it activates the parasympathetic nervous system, which is the part of your physiology that says we’re safe, stand down. If you’re trying to put on a CPAP mask while your nervous system is still in alert mode, you’re working against yourself. Five minutes of slow breathing first changes the conditions you’re putting the mask on under.
Other things people in the community use: guided meditation apps, white noise, progressive muscle relaxation, and just plain reading a book on the couch with the lights low for half an hour before bed. There’s nothing magic about any specific technique. The goal is the same. Arrive at the mask in a calmer state than you’d arrive at it in if you went straight from doom scrolling to bedtime.
My Wife, and the Practical Side of Living With CPAP
This is one of the few places where my own experience genuinely contributes. A decade in, my wife still tells me to put my mask on when she can hear me starting to drift off without it. That sounds small. It isn’t. Having someone who is on board with the therapy and quietly nudging you toward it makes the difference between consistent use and a lot of nights where the mask stays on the bedside table.
If you have a partner, it’s worth telling them what you’re going through with the equipment, what the alternative looks like (which is sleep apnea, untreated, with all the cardiovascular risk that comes with it), and what kind of support would actually help. For some people that’s a reminder. For some it’s silence and patience while you get the headgear adjusted. For some it’s just acknowledgement that yes, this is awkward at first, and yes, it’s worth it.
If you’re sleeping alone, the same role can be filled by a phone alarm at bedtime, a written note where you’ll see it, or any kind of cue that prompts you to actually start the routine on a night when you’d rather not. The hardest part of consistent CPAP use, after the equipment itself, is just the choice to put it on when you’re tired and don’t feel like dealing with it.
Track What’s Actually Happening
Modern CPAP machines record your usage hours, your apnea events per hour on therapy, your mask leak rate, and a few other variables. ResMed users see this in the myAir app. Other manufacturers have their own equivalents. The data is yours.
Why does this matter for anxiety specifically? Because what your body remembers and what your machine records are often different stories. People who feel like they had a terrible night often see four or five hours of clean data the next morning, with their AHI well under control. That’s not a trick. The mind tends to remember the moment you took the mask off in frustration at 3am much more vividly than the four hours of solid sleep that came before it.
Looking at your data each morning gives you a counterweight to the anxious part of your memory. It also tells you, over time, that the trend is moving in the right direction even when an individual night feels rough. For a lot of people in the community, this single habit is what gets them through the first month.
When CPAP Anxiety Isn’t Just CPAP Anxiety
Sometimes what feels like fear of the mask is something else.
If you’re having full panic attacks the moment you start the machine, or if the thought of the mask is keeping you awake long before bedtime, that’s beyond what gradual exposure on its own is designed to handle. It’s worth talking to your sleep clinic about whether what you’re dealing with is mask specific or whether you have an underlying anxiety pattern that the mask is triggering. Those have different treatments.
A 2023 systematic review in the journal Applied Nursing Research concluded that structured behavioral and psychosocial interventions, including cognitive behavioral therapy, produce meaningful improvements in CPAP use for people who struggle with the equipment. CBT for CPAP isn’t widely advertised, but sleep clinics can refer to clinicians who specifically work on it. If you’ve been working at this for six weeks and you’re not making progress, that’s a reasonable point to ask about it.
It’s also worth ruling out medical causes of physical discomfort. Untreated nasal congestion, a deviated septum, sinus issues, allergies, all of these can make CPAP miserable in a way that gets blamed on anxiety when really the body is just objecting to something fixable. The Mayo Clinic has a useful page on common CPAP problems and adjustments that covers a lot of the physical causes of trouble.
What Tends to Be True a Few Months In
The pattern I’ve watched play out in the community, over and over, is that people who get past the first month or two stop talking about the mask much. It becomes background. The thing that loomed so large at the start fades into a piece of equipment they put on without thinking, the same way you’d put on glasses.
That doesn’t mean it’s instant. It doesn’t mean everyone gets there at the same speed. Some people need three weeks. Some need three months. Some need professional support to get there at all. None of those timelines are wrong.
What stays consistent is that the people who keep showing up tend to keep getting better. The mask becomes routine. The morning headaches fade. The daytime fog lifts. At some point you realize the equipment that felt impossible has become the thing that lets you feel normal again.
For me, the migraine relief was so profound and so immediate that the alien on the face feeling never had time to become a real obstacle. If you’re interested in that side of the story, I’ve written separately about how CPAP changed the migraines I’d been having for years, and there’s a longer version of the early adjustment experience on the living with sleep apnea page. The companion guide to this one is how to get used to CPAP therapy, which goes into more detail on what the first few weeks tend to look like in general.
If you’re in the hard part right now, what I’d say, having watched a lot of people work through this, is that it’s worth giving the therapy a real shot. Slowly. With support. With a clinic who knows you’re struggling and can adjust things rather than telling you to push through. The mask is genuinely strange the first time. The benefits are genuinely real. Most people, given a fair chance and the right adjustments, end up on the other side.
Sources
Edmonds JC, Yang H, King TS, Sawyer DA, Rizzo A, Sawyer AM. Claustrophobic Tendencies and Continuous Positive Airway Pressure Therapy Non-adherence in Adults with Obstructive Sleep Apnea. Heart Lung. 2015 Mar-Apr;44(2):100-106. https://pmc.ncbi.nlm.nih.gov/articles/PMC4352200/
Mayo Clinic. CPAP machines: Tips for avoiding 10 common problems. https://www.mayoclinic.org/diseases-conditions/sleep-apnea/in-depth/cpap/art-20044164
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).