CPAP and Asthma: What I’ve Learned Living With Both Conditions

I’ve had asthma my entire life. It has just always been there, part of the background noise of breathing. My brother has it too, so it probably runs in my family.
So when I was diagnosed with severe obstructive sleep apnea more than a decade ago with an AHI of 51, I didn’t immediately think about the two conditions as related. I thought of them as separate problems. The sleep apnea was new and alarming. The asthma was just old and familiar.
What I’ve come to understand since then is that the two conditions are more intertwined than they might seem, and that CPAP therapy, the treatment that changed my life on the sleep apnea side of things, has some real and interesting implications for people who also live with asthma. I want to share what the research says about sleep apnea and asthma, and where my own experience fits in.
A reminder before we go further: I have a background in computer science, not medicine. Nothing here should be taken as medical advice. If you are managing both asthma and sleep apnea, your doctor and your sleep specialist are the right people to guide your treatment plan. What I can offer is a patient’s perspective and a reasonably careful read of the available evidence.
Are sleep apnea and asthma related?
It might surprise you how commonly asthma and obstructive sleep apnea occur together. A 2015 study in JAMA, drawing on the long-running Wisconsin Sleep Cohort, followed adults who were free of sleep apnea at the start and tracked who developed it over time. Over the first four-year window, 27 percent of people with asthma developed obstructive sleep apnea, compared with 16 percent of people without asthma, and longer asthma duration was tied to higher risk. In other words, asthma appears to raise the odds of later developing sleep apnea.
Researchers describe the broader relationship as bidirectional, which is a careful way of saying that having one condition raises your odds of the other, and that when both are present, each tends to worsen the other. A 2023 review in the Journal of Clinical Medicine that summarized the current evidence reached the same conclusion, noting that the prevalence of sleep apnea climbs as asthma severity increases. You can read that review through the National Library of Medicine.
Researchers are still working out the exact reasons for this overlap, but several mechanisms appear to be at play. Asthma is often accompanied by allergic rhinitis, which causes nasal congestion and obstruction. That congestion can push you toward mouth breathing, reduce airflow through the upper airway, and increase the likelihood of the airway collapsing during sleep, which is essentially what obstructive sleep apnea is.
Anatomy matters too. Asthma can be associated with a generally narrower upper airway, and in some people with enlarged tonsils or adenoids, all of which raise the risk of sleep apnea. There is also evidence that asthma can affect the neural control of the muscles in the breathing passages, further weakening the airway’s ability to stay open during sleep.
Mayo Clinic notes that chronic lung diseases such as asthma are recognized risk factors for obstructive sleep apnea, sitting alongside conditions like high blood pressure and type 2 diabetes in that list. If you have asthma and have not been assessed for sleep apnea, it is worth raising with your doctor, particularly if you are a heavy snorer, a mouth breather, or you wake unrefreshed despite what feels like a full night’s sleep.
I can’t point to a clean personal example here, because I was managing both conditions before I really understood either of them. But knowing what I know now, the fact that I was a chronic mouth breather with severe sleep apnea and lifelong asthma makes a lot of sense as a cluster.
Can sleep apnea cause asthma?
This is a question I see asked a lot, and the honest answer is that the science has not nailed down a one-way cause and effect. What the evidence does show is a strong association and a relationship that runs in both directions. Asthma appears to raise the risk of developing sleep apnea, as the JAMA work above suggests, and untreated sleep apnea appears to make asthma harder to control.
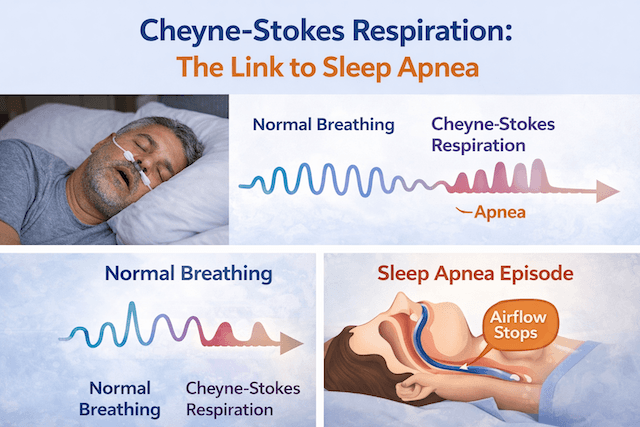
The mechanism on the sleep apnea side is worth understanding. When obstructive sleep apnea goes untreated, the airway repeatedly collapses through the night, oxygen levels swing up and down, and sleep fragments into dozens or hundreds of brief arousals. That repeated stress, along with the inflammation it provokes, can irritate airways that are already sensitive in someone with asthma. The Sleep Foundation’s overview of asthma and sleep notes that treating sleep apnea can often reduce asthma symptoms, which is one more reason to take the sleep apnea side of the picture seriously.
So rather than saying sleep apnea causes asthma, it is more accurate to say the two feed into each other. If you already have asthma, leaving sleep apnea untreated can make the asthma worse, and that is the part you actually have some control over.
What CPAP does, and doesn’t do, for asthma
CPAP is not an asthma treatment. That is worth saying clearly up front. Your inhaler, your preventer medication, your avoidance of triggers, none of that changes because you are on CPAP. The two treatment approaches sit alongside each other. One does not replace the other.
That said, there is legitimate evidence that CPAP therapy may have a positive secondary effect on asthma symptoms for people who have both conditions. The pressurized airflow from a CPAP machine keeps the upper airway open throughout the night. This prevents the repeated collapses that trigger arousals, oxygen drops, and the cascade of inflammation that follows. By stabilizing nighttime breathing, CPAP may reduce the airway irritation that can aggravate asthma. The research suggests this effect is most noticeable for people who have both poorly controlled asthma and severe sleep apnea, which, for the record, describes where I was at diagnosis.
There is also a more mechanical benefit. Modern CPAP machines pull air through a filter before delivering it. The air you are breathing all night has been filtered and, if you are running a humidifier, warmed and moistened. For someone with asthma who may be sensitive to dry air, cold air, or airborne irritants, that matters.
Can I say definitively that CPAP helped my asthma? Honestly, that is hard to untangle. I have had asthma so long that I do not have a clean baseline to compare against. What I can say is that my sleep changed dramatically after starting CPAP, and that on balance I feel better than I did. Whether any improvement in my breathing relates to the asthma specifically, or is simply the result of sleeping properly for the first time in years, I genuinely can’t say. I am not going to claim a connection I can’t verify.
Can an inhaler help with sleep apnea?
Since both conditions involve breathing, people sometimes wonder whether an asthma inhaler can do anything for sleep apnea. It is a fair question, and the answer is no. An inhaler treats asthma by relaxing the airway muscles or reducing inflammation in the lungs. Obstructive sleep apnea is a mechanical problem, where the upper airway physically collapses during sleep, and an inhaler does nothing to hold that airway open.
So an inhaler stays central to managing asthma, but it is not a treatment for sleep apnea. If you have both conditions, you treat both, with the right tool for each: inhaled medication for the asthma, and airway support such as CPAP for the sleep apnea.
What about BiPAP and asthma?
BiPAP, or bilevel positive airway pressure, comes up in asthma searches because it has a real role in one specific setting. In hospitals, a form of bilevel support is sometimes used as part of managing a severe asthma attack, helping a struggling patient move air while other treatments take effect. That is an acute, supervised use in a medical setting, and it is not the same as routine therapy at home.
For ordinary day-to-day breathing, a BiPAP machine is generally prescribed for certain forms of sleep-disordered breathing or for people who cannot tolerate standard CPAP pressures, not as a home treatment for asthma. I have not used a BiPAP myself, so I am describing it strictly from the literature rather than from experience. If a doctor is weighing CPAP against BiPAP for your situation, that is a conversation to have with them about your specific needs.
Humidification: where I do have something to say
One area where I can speak from experience is the humidifier. My ResMed AirSense 10 has a built-in humidifier, and I run it every night. The airflow feels comfortable, noticeably more so than I would imagine it being without it.
Dry air is one of the most common complaints from CPAP users, and it is particularly relevant for people with asthma, since cold or dry air is a known asthma trigger for many people. Breathing pressurized air all night through a machine that is not humidified can dry out the nasal passages and throat, which can irritate airways that are already sensitive.
The heated humidifier counteracts this. The AirSense 10 lets you dial in humidity levels, and with a heated hose, the air arrives warm and moist rather than cold and dry. This is not a cure for anything, but for anyone with asthma who is wondering whether CPAP is going to make their airways feel worse, a properly tuned CPAP humidifier is the answer to that concern. If you are starting CPAP and you have asthma, do not skip it. It makes a real difference to comfort and airway tolerance.
The full face mask question
This one is relevant to me specifically, and it may be relevant to you. I am a chronic mouth breather, and I have used a full face mask, the ResMed AirFit F20, since I started CPAP therapy. It is the only mask I have used.
For people with asthma, mask choice interacts with the condition in a couple of ways. Nasal masks and nasal pillow masks only work well if you can breathe through your nose consistently. If you have asthma with accompanying nasal congestion, rhinitis, or significant mouth breathing, a nasal mask can be frustrating, because when your nose is blocked or you open your mouth during sleep, you lose the pressure seal and the therapy becomes less effective.
A full face mask covers both nose and mouth, which means pressure is maintained regardless of which route air is moving. For mouth breathers with asthma, this is typically the more practical choice. That said, mask fit matters enormously. A poorly fitting full face mask can leak, which dries out your eyes and reduces the effectiveness of treatment. Getting the right size cushion and checking the seal regularly is worth the effort. If you are still figuring out which type suits you, I have written more on nasal versus full face CPAP masks.
Can CPAP make asthma worse?
It is fair to ask whether CPAP could aggravate asthma rather than help it. The honest answer is that in some circumstances, yes, it is possible, and the causes are usually fixable.
The most common culprit is unhumidified or inadequately humidified air. If the air coming through your machine is too dry or too cold, it can irritate sensitive airways. The fix here is humidification, as discussed above.
A poorly fitting mask that leaks around the seal can also contribute. Leaks mean the system is not properly pressurized, which reduces treatment effectiveness, and persistent leaks dry out the mouth and nasal passages in ways that can irritate the airways.
There is also the question of pressure. CPAP pressure is prescribed, and you should not adjust it yourself. If your prescribed pressure feels uncomfortable, or you find yourself fighting the machine, talk to your doctor. There are options like ramp settings, where the machine starts at a lower pressure and builds up gradually as you fall asleep, expiratory pressure relief, which eases the pressure slightly as you breathe out, or in some cases a switch to an APAP machine that adjusts pressure automatically through the night. These changes are your doctor’s call, but they are worth raising if you are struggling.
If you notice that your asthma symptoms are worse since starting CPAP, more coughing, more wheezing, or a generally more irritated airway, that is a conversation to have with your doctor rather than something to manage on your own.
Keeping your equipment clean matters more when you have asthma
People with asthma have particular reason to be diligent about equipment hygiene. A CPAP machine that is not cleaned regularly can harbor bacteria, mold, and dust, exactly the kinds of airway irritants that asthma patients need to minimize. The humidifier water chamber in particular is a warm, moist environment that can allow bacterial growth if it is not cleaned and refilled with fresh distilled water daily.
The manufacturer’s guidelines on cleaning frequency exist for a reason. Warm water and mild soap for the mask and water chamber, plus regular filter checks and replacements, is basic maintenance, but it is worth taking seriously if asthma is part of your picture. This becomes even more important when you are run down with a cold or chest infection, which is exactly when an asthma flare can ride along, and I have written separately about using CPAP when you are sick.
One note on ozone based CPAP cleaners: the FDA has raised concerns about these devices, and they are generally not recommended. Ozone residue left in the mask or tubing is an airway irritant that you do not want to be breathing all night, particularly if your airways are already sensitive.
When to talk to your doctor
If you have asthma and you are being assessed for sleep apnea, or if you have sleep apnea and asthma is already part of your history, it is worth making sure both your sleep specialist and the doctor managing your asthma are aware of both conditions. They interact in ways that can affect treatment decisions on both sides.
Specifically, tell your team if your asthma symptoms seem to have changed since starting or stopping CPAP, if you are experiencing significant dryness, coughing, or airway discomfort with CPAP use, if you are having trouble tolerating the pressure, or if your asthma is poorly controlled and you have not been assessed for sleep apnea. Because the two conditions can reinforce each other, treating the sleep apnea may support better overall asthma management.
Further reading
For more on the connection between asthma and disrupted sleep, the Sleep Foundation has a detailed overview of asthma and sleep. And for a thorough look at what obstructive sleep apnea is, including its risk factors and how asthma fits into that picture, Mayo Clinic’s page on obstructive sleep apnea symptoms and causes is worth bookmarking.
If you want to understand how sleep apnea severity is measured, my page on the AHI, or apnea-hypopnea index, explains what those numbers mean and why they matter. My AHI at diagnosis was 51, which put me firmly in the severe category.
The bottom line
Living with both asthma and obstructive sleep apnea is common, and the two conditions interact in meaningful ways. CPAP therapy is not an asthma treatment, but for people who have both, the evidence suggests it may support better asthma control by stabilizing nighttime breathing and reducing the airway inflammation that comes with untreated sleep apnea.
Humidification is important, arguably more so for people with asthma than for those without. Mask fit matters too, particularly if you are a mouth breather. And keeping your equipment clean is not optional.
I have had asthma my whole life, and I have been on CPAP for more than a decade. Whether the CPAP has helped the asthma directly, I genuinely can’t say. But breathing through a well-fitted mask with warm, filtered, humidified air every night has never made my asthma worse. And for a condition I have managed my entire life, that is something.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).