Chiari Malformations and Sleep Apnea: A CPAP User’s Notes
The first time I saw “Chiari” come up in a CPAP discussion online, I had to look it up. Someone in the thread had been diagnosed with one and was asking the group whether their pressure setting needed adjusting given the structural issues at the base of their skull. I had been on therapy for the better part of a decade at that point and had never heard of it. So I went and read.
What follows are my notes from that reading, written for anyone in the CPAP community who has run into the term and wants a layperson’s overview of what it is, why it keeps surfacing in sleep apnea conversations, and where the topic intersects with the world most of us actually live in.
I want to be upfront before I go any further. I do not have a Chiari malformation. I am not a neurologist or a sleep physician. My background is in computer science and my experience with sleep medicine starts and ends with my own obstructive sleep apnea, diagnosed with an AHI of 51 more than a decade ago. If you have landed here trying to make sense of an actual Chiari diagnosis, please talk to a specialist. The point of this article is more modest.
What a Chiari Malformation Actually Is
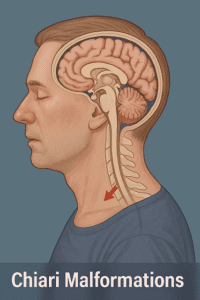
A Chiari malformation is a structural problem at the base of the skull. In a typical anatomy, the cerebellum, the part of the brain that handles balance and coordination, sits entirely inside the skull. In someone with a Chiari malformation, part of the cerebellum extends downward through the foramen magnum, the opening at the base of the skull where the spinal cord exits, and pushes into the upper spinal canal. The Mayo Clinic describes it as a condition in which brain tissue extends into the spinal canal, often because the skull is misshapen or smaller than typical, pressing on the brain and forcing it downward.
There are several types. Type 1 is the most common and the one most relevant to a sleep apnea audience because it often goes undiagnosed until adulthood. Symptoms can develop slowly and can be vague enough to be mistaken for migraines, anxiety, or general fatigue. Types 2, 3, and 4 are progressively more severe and are usually identified in infancy or before birth. For the rest of this article I will mostly be talking about type 1, since that is the type adults are most likely to encounter.
The condition is not as rare as it once seemed. MRI has become routine for everything from headaches to neck pain, and incidental findings of mild Chiari malformations are increasingly common. Many people who have one will never develop significant symptoms. Others will have a lifetime of headaches, balance problems, and odd neurological complaints before anyone connects the dots. That gap, between having the condition and having it recognized, is part of why the sleep apnea community keeps bumping into it.
Why It Keeps Coming Up in Sleep Apnea Conversations
The sleep apnea connection is real and it has a clear mechanism. The brainstem, which sits just above the spinal cord and below the cerebellum, contains the respiratory control centers. These are the cells that send rhythmic signals telling the diaphragm and chest muscles to contract and pull in a breath. When the cerebellum herniates downward, it can compress or distort the brainstem. Compress the wrong cells and the signal to breathe gets disrupted.
This is what produces central sleep apnea, and it is why people with Chiari malformations are at higher risk for it than the general population. Central sleep apnea is fundamentally different from the obstructive sleep apnea I have. In OSA, the airway physically collapses while the brain is still trying to breathe. In central apnea, the airway is open and the breathing muscles are willing, but the signal from the brain stops arriving. The Sleep Foundation describes it as a disorder defined by pauses in breathing due to a lack of respiratory effort during sleep.
There is also an obstructive component that can show up in some Chiari patients. Structural differences at the skull base and upper neck can affect the geometry of the upper airway, making it more prone to collapse. People with anatomical contributors to apnea, whether that is a small jaw, a crowded oropharynx, or a structural skull issue, can end up with sleep disordered breathing for reasons that have nothing to do with weight or soft tissue alone. I have written separately about micrognathia and obstructive sleep apnea as another example of the same general theme.
So the picture is messier than a simple either or. A given person with Chiari might have central apneas, obstructive apneas, or a mix of both. That mix matters because it changes what treatment will and will not help.
Where My Story Connects, and Where It Does Not
I want to be careful here, because this is the part where it would be easy to overreach.
When I was diagnosed, I was waking up most mornings with a heavy, dull headache. The kind that sat behind my eyes and took half the morning to lift. Once I started CPAP, those headaches faded. I have written about that experience in detail in my piece on sleep apnea and migraine headaches. For me, the headaches were a downstream symptom of the apnea itself. Fix the breathing, fix the headache. Simple.
For someone with a Chiari malformation, the headache equation is not simple. Chiari headaches have a distinct pattern that doctors look for. They are typically located at the back of the head. They are often triggered or made worse by coughing, sneezing, straining, or bending forward. They do not respond to the same treatments that resolve apnea driven headaches, because they are caused by mechanical pressure and disrupted cerebrospinal fluid flow, not by oxygen desaturation overnight.
This is the practical takeaway I would want anyone reading this to walk away with. If you have started CPAP and your AHI has dropped to a healthy range but your morning headaches are still there, especially if they have that cough and strain trigger pattern, that is worth raising with your doctor. The CPAP did its job. Something else is causing the headaches. It might be a million things, most of them not Chiari, but Chiari is on the list of things a thorough workup will consider.
The reverse warning matters too. If you have been on therapy for a while and your machine data shows a high number of central events, sometimes called clear airway events on ResMed reports, that is a conversation to have with your sleep clinician, not something to figure out alone. Most central events on a CPAP report have ordinary causes, including treatment emergent central apneas that resolve on their own as the body adapts to therapy. But persistent central events without an obvious explanation are one of the patterns that sometimes lead to imaging.
How Chiari and Sleep Apnea Get Diagnosed Together
If a doctor suspects Chiari, the diagnostic path runs through MRI. It is the only imaging study that reliably shows the position of the cerebellar tonsils relative to the foramen magnum and quantifies the herniation. CT scans can sometimes hint at it but do not show the soft tissue clearly enough to confirm the diagnosis.
The sleep apnea side of the workup runs through a sleep study, which is the same study most readers of this site will already be familiar with. An overnight polysomnography is the gold standard because it can distinguish obstructive events from central events, monitor brain activity, and measure how breathing changes across sleep stages. I have written about what to expect from a sleep study elsewhere on the blog. For someone being evaluated in the context of a known or suspected Chiari malformation, the sleep study takes on particular importance, because the breakdown between obstructive and central events directly informs treatment choices.
A few patients end up doing the workup in the opposite order. They get the sleep study first because of daytime sleepiness or a partner’s report of pauses in breathing. The study comes back showing an unexpectedly high proportion of central events. The sleep physician asks the right questions, and an MRI follows. This is part of why a thorough sleep clinician will ask about headaches, neck pain, balance, and family history during the intake conversation. The answers can change the picture.
Treatment Is More Complicated Than CPAP
For straightforward obstructive sleep apnea like mine, the treatment conversation is relatively simple. CPAP is the first line, the equipment is well understood, and the path from diagnosis to a working setup is reasonably predictable. I have used my own ResMed AirSense 10 for the better part of a decade and I have a clear sense of what good therapy looks like for my body.
For someone with Chiari, the treatment conversation has more branches.
Surgery is one branch and is the only intervention that addresses the underlying cause. The procedure most often used is called posterior fossa decompression. A neurosurgeon removes a small section of bone at the back of the skull, sometimes also a piece of the top vertebra, to create more room for the cerebellum and relieve pressure on the brainstem. When central apneas are clearly being caused by brainstem compression, decompression can reduce or resolve them. It is a serious operation, not a casual one, and it is reserved for cases where symptoms warrant it. The decision to operate sits with a neurosurgeon and the patient, weighing severity of symptoms against surgical risk.
Positive airway pressure is the other branch and is often used either alongside surgery or in place of it, depending on the person. CPAP can help if there is an obstructive component, in the same way it helps the rest of us. Adaptive servo ventilation, usually called ASV, is a different category of machine designed specifically for some types of central apnea and certain breathing patterns. ASV machines monitor the patient’s breathing and adjust pressure dynamically to stabilize the rhythm. ASV is not a machine I use or have personal experience with, so I will not pretend otherwise. If you have been told you might need one, the conversation to have is with your sleep physician, not with a CPAP user on the internet.
Lifestyle measures, weight management, and treating any contributing conditions still matter, the same way they matter for any sleep apnea patient. They do not replace structural treatment when the structural problem is the cause, but they do not become irrelevant either.
What I Would Take Away From All of This
If you have read this far and you do not have a Chiari malformation, here is what I would take away from a few weeks of reading on this topic.
First, the structural causes of sleep apnea are real and they deserve more attention than the standard CPAP narrative gives them. Most of us think of sleep apnea as a soft tissue and weight problem. Sometimes it is. Sometimes it is not. Conditions like Chiari malformation, micrognathia, and other anatomical issues can drive apnea in ways that the standard treatment script does not fully address.
Second, symptoms that do not resolve on CPAP are worth investigating rather than ignoring. CPAP is remarkably good at fixing what it is supposed to fix, which is the breathing interruption itself. If something else stays broken after months of solid therapy, the CPAP is not failing. The diagnosis might just be incomplete.
Third, machine data is useful but not diagnostic. A pattern of central events on your nightly report is a signal to ask your clinician questions, not a verdict. Forums are good for orienting yourself and finding the right questions to ask. They are not a substitute for the doctor who can look at the data alongside everything else they know about your body.
And fourth, the people in CPAP forums and groups who bring up conditions like Chiari are often more clued in than the broader community gives them credit for. The person whose post sent me down this rabbit hole had clearly spent years putting together their own picture of what was happening to them. That kind of self advocacy is part of why sleep medicine has gotten better at recognizing these less common patterns. It pays to listen.
Closing Thoughts
If you came to this article looking for a guide to managing a Chiari diagnosis, I hope it is clear by now that I am not the right person to write that guide. What I can offer is one CPAP user’s reading of why Chiari keeps surfacing in our conversations, and a small map of where the topic intersects with the world I do know firsthand.
If you have questions, leave a comment. If you have a Chiari diagnosis and want to share what your sleep study and treatment path looked like, I would genuinely like to hear it, both because I would learn from it and because future readers will too. The CPAP community has always been at its best when patients teach each other what the appointment slots and pamphlets do not have time to cover.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).