Aerophagia and Sleep Apnea: What Ten Years of CPAP Taught Me About Swallowing Air
If you have ever woken up feeling like someone inflated a beach ball inside your stomach overnight, you already have a pretty good sense of what aerophagia feels like. It’s that strange, heavy, full belly sensation that has nothing to do with what you ate for dinner and everything to do with the machine sitting on your nightstand. After more than a decade on CPAP therapy for severe sleep apnea, I have been through this side effect more times than I care to count, and I have picked up a lot of hard won lessons about what actually helps and what is just repeated filler advice.
Aerophagia is the medical word for swallowing air. In the CPAP world, it sometimes gets called “CPAP belly,” which is the kind of name only a sleep clinic nurse could come up with. Whatever you call it, it is uncomfortable, occasionally embarrassing, and for some people it becomes the reason they quietly give up on their therapy. I don’t want that to happen to you, so let me walk you through what it is, why your machine is doing this to you, and the exact things that worked for me over the years.
What Aerophagia Actually Feels Like
Clinical pages describe aerophagia as “excessive swallowing of air leading to gastrointestinal symptoms.” That is accurate, but it doesn’t capture the morning of it. For me, the first sign was always the same: I would wake up, take off my mask, sit up, and immediately let out a burp that could have rattled the windows. Then another. Then a third. By the time I made it to the kitchen, my stomach felt bloated and tight, and I had that uncomfortable cramping that comes from trapped gas that just cannot decide which end it wants to leave from.
Why CPAP Therapy Causes Aerophagia in the First Place
The classic symptoms are bloating, belching, flatulence, upper abdominal cramping, and sometimes a reduced appetite at breakfast because your stomach is already full of air from your machine. Some people also notice a bit of regurgitation or mild reflux, especially if they already had GERD before starting therapy. The first time it happened to me, I honestly thought I had picked up a stomach bug. It took a conversation with my sleep clinician to realize the CPAP was the source.
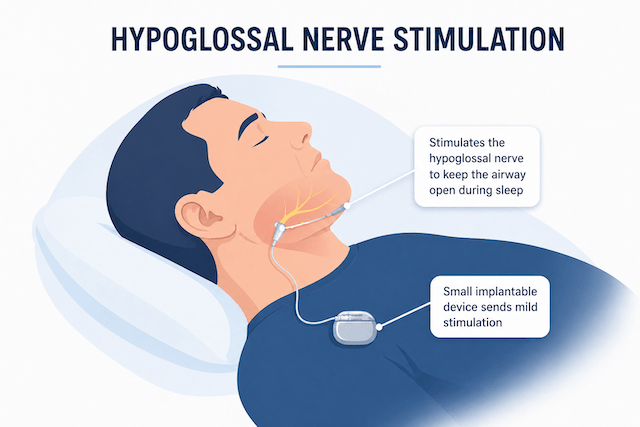
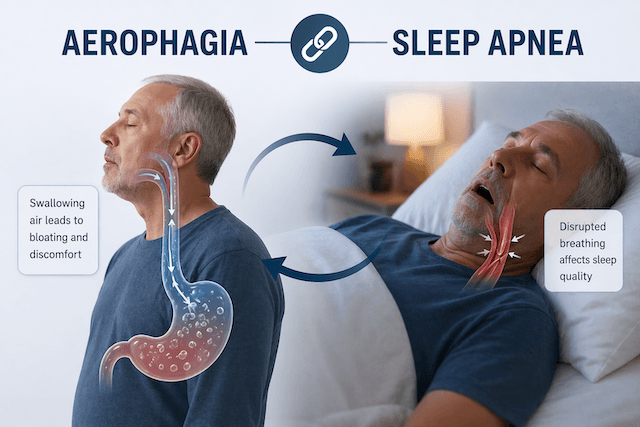
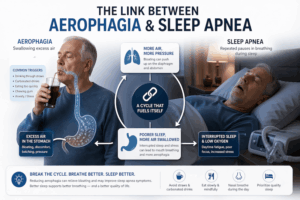
The mechanism is more interesting than most blogs make it sound. When you breathe normally at night, your upper esophageal sphincter stays mostly closed. It’s a ring of muscle at the top of your esophagus whose whole job is to keep air and food out when they are not supposed to be there. But during deep sleep, particularly slow wave sleep, that sphincter relaxes. At the same time, your CPAP is blowing pressurized air at your face all night long.
Most of that air goes where it is supposed to go, down into your lungs. But if the pressure is high enough, or if you are mouth breathing, or if you are sleeping on your back with your head tilted a certain way, a portion of that air slips past the sphincter, travels down the esophagus, and ends up in your stomach. Once it’s there, your stomach has exactly two options for getting rid of it, and neither one is subtle.
The Cleveland Clinic explains the mechanism clearly and notes that any time your body takes in more air than it can release, you feel it. With CPAP, the machine can push more air in than your digestive tract can reasonably offload, which is why the symptoms tend to cluster in the first few hours after waking.
There is also a strong link between aerophagia and gastroesophageal reflux. Research published in the sleep medicine literature has shown that a significant portion of CPAP users who develop aerophagia also have GERD, and the two seem to feed each other. If you already have reflux, your lower esophageal sphincter is probably not as tight as it should be, which makes it easier for air to move between your stomach and esophagus in both directions. This is one of the reasons I always ask people with stubborn aerophagia whether they have any reflux symptoms, because treating one can dramatically improve the other.
A Helpful Video Explanation
If you want a visual breakdown of what is happening, Jason over at axgsleepdiagnostics has a good YouTube explainer on aerophagia. It covers the airway anatomy in a way that helped me understand what my own body was doing all those nights. Worth a watch if you are the kind of person who wants to see how the pieces fit together.
How Common Is This Really?
The Sleep Foundation estimates that somewhere between 16 and 50 percent of CPAP users experience aerophagia at some point. That is a huge range, and it tells you how much the condition depends on individual factors like your anatomy, your pressure setting, your mask type, and whether you have reflux.
Here is the part most people don’t realize. A lot of CPAP users who quit therapy within the first ninety days do so because of aerophagia, and they often never tell their doctor. They just stop using the machine and assume CPAP is not for them. I nearly did this myself in my second year. I went two weeks bloated, groggy, and discouraged before I finally picked up the phone and asked my respiratory therapist whether this was normal. Turns out it was, and more importantly, it was fixable.
My Own Journey With CPAP Belly
When I first started therapy, I was on a fixed pressure of around 12 cmH2O on an older Philips machine, with a full face mask because I was a confirmed mouth breather. My AHI dropped dramatically, my wife stopped elbowing me at night, and everything was looking great except for the stomach.
Every morning I had that familiar inflated feeling. Some days it was mild, other days it was bad enough that I would skip breakfast. After about a month, I started tracking it. I wrote down my pressure, my mask, my sleeping position, and the severity of my symptoms each morning. That simple exercise taught me more than any website did, because I started seeing patterns. The worst mornings came after nights when I slept flat on my back and when I had eaten late the night before. The best mornings came when I slept on my side with my head slightly elevated and had finished dinner at least three hours before bed.
That was the start of fixing it. Over the years, I have worked through a handful of adjustments, and at this point my aerophagia is rare enough that I almost forget it was ever a problem. Almost. If you are dealing with the same thing, here is what I would try in order.
Get Your Pressure Settings Right
This is the single biggest lever. The higher your prescribed pressure, the more force the air has to push past your upper esophageal sphincter, especially during the deeper stages of sleep. If you are running at the top end of the CPAP range and you are struggling with aerophagia, your clinician may be able to drop the pressure a notch or two without compromising your AHI.
That said, don’t start fiddling with the machine yourself. I have written before about how CPAP pressure settings need to balance treating your apnea with keeping you comfortable, and that balance is individual. Ask your sleep doctor to pull your most recent data and see whether your pressure is genuinely needed at the level you are on, or whether it could safely come down. In my case, moving from a fixed 12 to an auto ranging setup with a lower minimum made a massive difference. My stomach thanked me.
Consider Switching From CPAP to APAP or BiPAP
This was my second big breakthrough. A standard CPAP delivers one constant pressure all night. An APAP machine adjusts pressure in real time based on what your airway is doing, which means it only hits high pressures when you actually need them. For a lot of the night, you get lower pressure and less air getting swallowed.
BiPAP is another option, and for some people it is the real game changer. It delivers a higher pressure on the inhale and a lower one on the exhale, which means you spend half of every breath at a pressure that is much less likely to push air into your stomach. If you want to understand the differences in more detail, I put together a full breakdown of CPAP versus BiPAP that goes through when each one makes sense. If your aerophagia is severe and you are already on a high CPAP pressure, this is a conversation worth having with your specialist.
Look Hard at Your Mask
Your mask matters more than almost anyone tells you. A full face mask covers your nose and mouth, which keeps you treated even if you breathe through your mouth, but it also makes it easier for air to end up in your stomach because you are essentially being pressurized from two entry points. Research and clinical experience both suggest that nasal masks and nasal pillow masks tend to reduce aerophagia compared to full face designs.
I switched from a full face mask to a nasal pillow setup about five years into my CPAP journey, and the difference in morning bloating was noticeable within a week. I still use a full face mask when I have a cold and my nose is blocked, but for everyday use, nasal pillows are my default. I went into the trade offs in more detail in my comparison of nasal versus full face CPAP masks if you want to see where each one shines.
Of course, if you are a mouth breather, moving to a nasal mask brings its own challenges, because the air has to go somewhere. Which brings me to the next point.
Address Mouth Breathing
If your mouth falls open at night, your CPAP air has a much easier path into your stomach, because the air that should be going through your nose into your airway instead takes the scenic route past your tongue and straight into your esophagus. A chin strap can help, and for some people mouth taping works well. I have tried both over the years. The chin strap felt a bit silly the first week but quickly became part of my routine, and it made my therapy noticeably more effective.
There is also a connection between chronic mouth breathing and broader health issues, which is something I wrote about in my piece on mouth breathing, sleep apnea, and low testosterone. Solving the mouth breathing problem almost always helps the aerophagia, and it helps a lot of other things at the same time.
Change Your Sleeping Position
Sleeping flat on your back is the worst position for aerophagia. When you are on your back, gravity is no longer helping air stay in your upper airway, and any air that slips past the sphincter has a clear downhill path into your stomach. Side sleeping, particularly on your left side, is almost always better. It makes it harder for air to pool in your stomach and it reduces reflux at the same time.
I learned this the hard way on nights when I would fall asleep on my side and wake up at 3 a.m. on my back. The bloating the next morning was always worse on those nights. I now use a body pillow to keep me anchored on my side, and I sleep with the head of the bed slightly elevated. Those two changes alone cut my aerophagia symptoms in half.
Watch What You Do Before Bed
Eating late, drinking carbonated beverages in the evening, chewing gum right before bed, and even heavy conversation at dinner can all increase how much air you have already swallowed before you put on your mask. Once the CPAP starts adding to that baseline, you are in trouble. I try to finish eating by about three hours before bed, skip the fizzy drinks after dinner, and avoid anything that triggers reflux. None of this is dramatic, but the cumulative effect is real.
Alcohol is another one worth mentioning. It relaxes the same sphincters that are supposed to keep air out of your stomach, and it can make aerophagia dramatically worse. A glass of wine with dinner is usually fine. Three beers right before bed is not.
Give It Time
Here is something most pages don’t mention. For a lot of us, CPAP related aerophagia gets better on its own over the first six to twelve months of therapy. The theory is that the muscles involved in controlling air flow in your upper airway gradually adapt to the nightly pressure, almost as if they are doing a slow resistance workout every time you sleep. I noticed this in my second year. Mornings that used to be miserable just stopped being so bad, without me doing anything new. So if you are in the early months and everything I have written above has not quite fixed it, there is a decent chance time will do some of the work for you.
That said, “give it time” is not an excuse to suffer. If your symptoms are severe or they are making you want to quit therapy, talk to your doctor now. Aerophagia is a solvable problem, and the sooner you start adjusting things, the sooner you get to enjoy the actual benefits of treating your sleep apnea.
When Aerophagia Is Worth a Doctor’s Visit
There are a few situations where you should stop troubleshooting on your own and just make an appointment. If your bloating is painful rather than just uncomfortable, if you have unexplained weight loss alongside the symptoms, if you are vomiting or dealing with ongoing reflux, or if your symptoms started suddenly and got worse instead of better with CPAP use, those are not standard aerophagia stories. Your clinician can rule out other gastrointestinal issues and look at whether your therapy needs a real redesign rather than a tweak.
There is also a related issue worth flagging. CPAP users sometimes experience burping on a completely different scale than normal aerophagia, and the reasons are not always obvious. I covered that in more detail over at my article on why your CPAP might make you burp, which overlaps with this topic but is not identical.
For a more detailed clinical overview of the condition outside my own experience, the SleepApnea.org guide to aerophagia is worth bookmarking. They cover the research side more formally than I do and update their page regularly.
The Bottom Line
Aerophagia is annoying, sometimes painful, and almost always solvable. If you are in the thick of it right now, I want you to know three things. First, you are not broken, and this does not mean CPAP is wrong for you. It just means one or more of the variables in your therapy needs adjusting. Second, the fix is almost always some combination of pressure tweaks, mask change, position change, and reducing mouth breathing. Third, it really does tend to get better over time.
I came very close to quitting CPAP in my first two years because of this. I am glad I didn’t. Today my therapy is something I barely think about most nights, my AHI is exactly where it should be, and the morning bloating is a memory rather than a routine. If I can get there, you can too. Be patient, keep notes, talk to your clinician, and give yourself permission to experiment.
Thanks for reading. If this helped, stick around and have a browse through the rest of the blog. There are plenty more articles on the side effects nobody warned us about and the small adjustments that make a decade of therapy genuinely livable.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).