CPAP Sleep Study: What to Expect from an In-Lab or Home Sleep Test

A CPAP sleep study is the diagnostic test that decides whether you have sleep apnea, how severe it is, and whether CPAP therapy is the right next step. There are two main kinds: an in-lab polysomnography, usually shortened to PSG, and a home sleep apnea test, usually shortened to HSAT. Both produce the number that ends up driving everything else: your apnea-hypopnea index, or AHI.
This page is the practical version of the topic. What each test involves, what the results mean, what the path looks like after a diagnosis, and a few honest notes from someone who has been on the patient side of this for the better part of a decade.
A quick note on me before going further. I write from the patient side, not the clinical side. My background is in computer science, not medicine, so nothing on this page is medical advice. I was diagnosed with severe obstructive sleep apnea more than a decade ago through a home sleep test, and my AHI at diagnosis was 51. The longer story of how that diagnosis came together lives on my Living with Sleep Apnea page rather than this one.
The two types of CPAP sleep study
There are two ways to get a sleep apnea diagnosis. They serve different purposes and they capture different amounts of data.
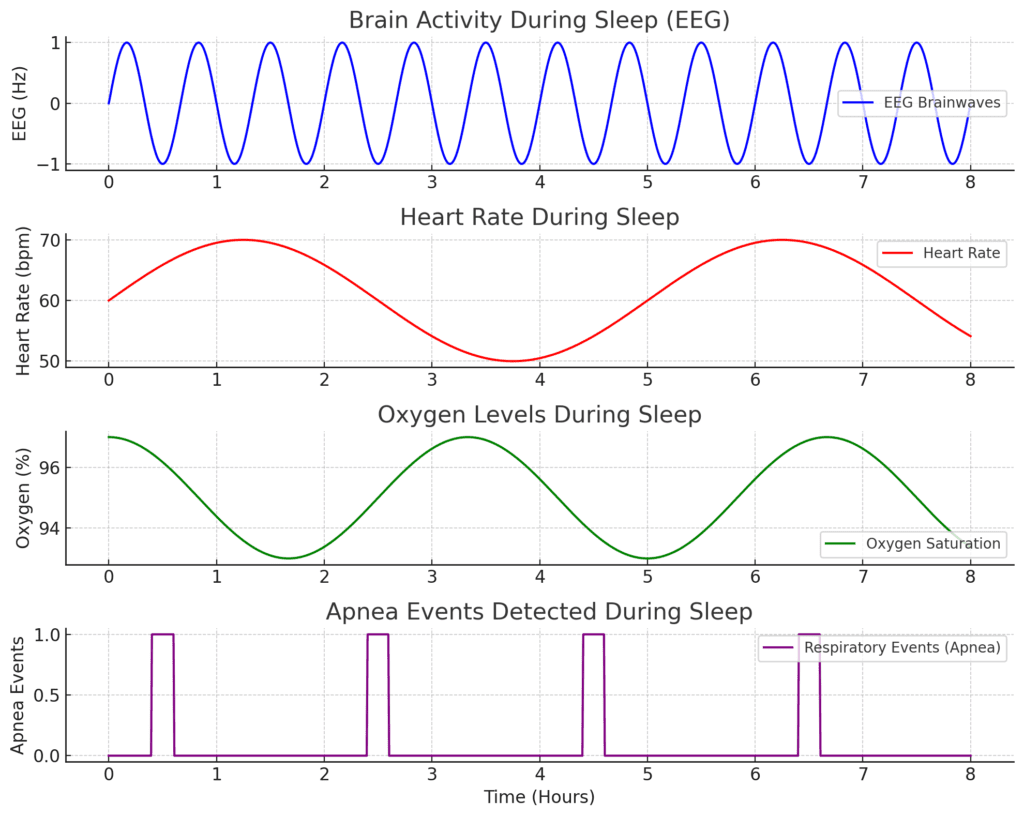
A polysomnography is the in-lab option. You spend a night in a sleep center while a sleep technologist attaches sensors to your scalp, face, chest, and legs. The recording captures your brain waves, eye movements, muscle tone, heart rhythm, breathing effort, airflow, and oxygen saturation. The American Academy of Sleep Medicine considers PSG the reference standard for diagnosing sleep apnea and other sleep disorders, and you can read the AASM patient overview of a sleep study here if you want their version of the explanation.
A home sleep apnea test is simpler. You collect the device from a clinic or have it shipped, set it up in your own bedroom before bed, and sleep at home. The device records a smaller set of signals: airflow, breathing effort, oxygen saturation, and heart rate or pulse. It does not record brain waves, which means it cannot tell precisely when you were asleep or what stage of sleep you were in. That tradeoff is what makes it cheaper, faster, and a lot more comfortable, but it also limits it to people whose history strongly suggests moderate to severe obstructive sleep apnea and who do not have other complicating conditions.
Either test can lead to a CPAP prescription. Which one your doctor orders depends on your symptoms, your medical history, the resources available where you live, and your insurance.
What I went through
I had a home sleep test. There were a lot of wires and sensors to attach and plug in by myself, more than a modern home test requires. Compare what I did to something like the WatchPAT One, which is a small wrist and finger device, and the older home rig I used felt closer to a stripped-down lab study at the kitchen table. The general guide on home testing is on my at-home sleep apnea test page if you want the wider picture.
The result came back severe. My AHI was 51, which meant I was averaging more than 50 breathing disruptions every hour of sleep. A clinician set my initial CPAP pressure based on the diagnostic data, and I started therapy at home.
That part deserves an honest note. The pressure they set the first time around was too high for me. The early mornings were rough. I felt drained, and I could feel the strain on my heart. I went back, asked for the pressure to be lowered, and once it was dialed in I started to feel real recovery. CPAP therapy is not a one-and-done setting. If something feels wrong in those first weeks, you go back. The emotional side of those first weeks is its own subject, and I cover it on my CPAP anxiety page.
What happens during an in-lab polysomnography

If your doctor refers you for a PSG, this is the rough shape of the night.
You arrive at the sleep center in the early evening, usually a couple of hours before your normal bedtime. The room is set up like a quiet hotel room: bed, lamp, private bathroom, sometimes a TV. You change into your own pajamas, fill out a brief intake about your day, and the technologist begins applying sensors.
The sensors are glued or taped to your skin. Some go on your scalp to record brain activity. Others go around your eyes for eye movement, under your chin for muscle tone, and on your chest for heart rhythm. Bands wrap around your chest and abdomen to track breathing effort. A small clip or sensor on your finger records oxygen saturation. A thin tube under your nose tracks airflow. Once everything is hooked up, the wires bundle into a single port so you can roll over without getting tangled.
The technologist watches the recording from another room. Most labs also use a low-light video camera and a microphone so they can see and hear snoring, gasping, or unusual movements. You read or watch TV until you feel sleepy, then they turn the lights out.
If your apnea is moderate to severe, the night may turn into a split night study. The first half captures your untreated sleep so a doctor can score your AHI. The second half puts you on CPAP, with the technologist gradually adjusting the pressure to find the lowest setting that keeps your airway open. The second half is called titration, and there is a separate write-up on CPAP titration if you want the longer version.
You usually leave by mid morning. The full report comes back within a week or two, depending on the lab.
What happens during a home sleep apnea test
A home sleep test is a much smaller production. The exact setup depends on the device, but the general shape is the same.
You receive the device the day of your test. Some clinics walk you through it in person, others rely on printed instructions and a setup video. The test is meant to be done on a normal night in your own bed, eating your normal dinner, going to bed at your normal time. You attach the sensors yourself: typically a finger sensor for oxygen, a small belt or chest strap for breathing effort, and a nasal cannula for airflow. Newer devices like the WatchPAT family use a wrist unit and a finger sensor instead of belts and cannulas, which is a real comfort upgrade.
You sleep, the device records, and in the morning you turn it off and return it. The data is downloaded, scored, and reviewed by a sleep physician. Because the device cannot tell exactly when you were asleep, the score from a home test is sometimes called a respiratory event index, or REI, and it can read slightly lower than a lab AHI because it averages events over total recording time rather than total sleep time. That is one reason a borderline negative home test is often followed by a referral for an in lab study.
The advantages of a home test are obvious. You sleep in your own bed. There are far fewer wires. The cost is lower. The wait is usually shorter. The disadvantage is that the test is narrower in what it can detect. If the clinical picture is anything other than straightforward suspected obstructive sleep apnea, a lab study is usually the better starting point.
What the results actually show
Whichever test you do, the report comes back full of acronyms. Here is what the important ones mean.
AHI, the apnea-hypopnea index, is the count of complete or partial breathing events per hour of sleep. Five to fifteen is mild, fifteen to thirty is moderate, and thirty or above is severe. The longer breakdown lives on my AHI page. The AHI is the headline number on most reports and is what insurance and prescribing decisions are usually anchored to.
ODI, the oxygen desaturation index, is how often your blood oxygen drops below a threshold per hour. It tells the clinician how hard the apnea is hitting your body, not just how often it is happening.
Sleep staging only appears on a PSG report, because brain wave recording is what makes it possible. It shows how much time you spent in light sleep, deep sleep, and REM sleep. People with untreated obstructive sleep apnea often spend most of the night stuck in light sleep, which is a big part of why daytime exhaustion and brain fog are so common.
Arousals are short awakenings your brain registers even though you do not consciously remember them. A high arousal index helps explain why someone with apnea can sleep eight hours and still feel like they have not slept at all.
The body of the report is dense, but a sleep physician will summarize it in plain language at your follow up. If they do not, ask. You are entitled to understand what your own data is telling you.
When to ask your doctor about a sleep study
You do not need a confirmed diagnosis to start the conversation. The signs that should at least make you raise the question with your doctor are well documented. Loud and frequent snoring. Witnessed breathing pauses. Waking up gasping or choking. Daytime sleepiness despite a full night in bed. Morning headaches. Difficulty concentrating. High blood pressure or atrial fibrillation, both of which can be linked to untreated apnea. The longer write-up is on my obstructive sleep apnea page.
In my case it was my wife who spotted it. She watched me stop breathing in my sleep and pushed me to act. That is a very common pattern. People with apnea rarely notice it themselves, because by definition they are unconscious for the events.
How to prepare for a sleep study
Whether your test is in a lab or at home, the prep is roughly the same. Avoid caffeine after the early afternoon on the day of the study. Caffeine has a long half life and can change how you sleep without you noticing. Skip naps that day. Avoid alcohol, which suppresses arousal responses and can muddle the reading.
For an in lab study, pack like a short hotel stay: pajamas, toiletries, your own pillow if you sleep best on it, something to read while you wind down, and a change of clothes for the morning. Take your normal medications unless your doctor has told you to pause something specific.
For a home test, give yourself time to read the setup instructions before you are tired. Set the device up in your bedroom while you are still alert. If anything is unclear, call the clinic before bedtime, not from bed at midnight.
What if the results come back negative or unclear
It happens. A single night does not always capture a representative sample of your sleep. If the report is borderline, your doctor may order a repeat study, switch you from home testing to in lab PSG, or add other tests like a multiple sleep latency test if narcolepsy is part of the differential. A negative home test followed by a confirmatory in lab study is a recommended pathway in current AASM diagnostic guidelines. If you came in with strong symptoms, do not let one inconclusive test be the end of the conversation.
Mayo Clinic publishes a clear plain language overview of polysomnography that is worth reading if you are nervous about what the in lab night involves.
What happens after a positive diagnosis
If the report shows obstructive sleep apnea, the most common next step is a CPAP prescription. CPAP, continuous positive airway pressure, is a small bedside machine connected by a hose to a mask you wear at night. The machine pushes a steady stream of air that holds your upper airway open while you sleep, which prevents the soft tissue collapses that cause apneas in the first place.
The prescription will include a pressure setting. In my case the clinician set the pressure based on my diagnostic data, and I started CPAP at home. When the first setting was too high I went back and had it adjusted. In other cases the prescription comes out of an in lab titration night, where the pressure is fine tuned in real time. Most modern machines also self adjust within a prescribed range over time.
CPAP is genuinely life changing once it is dialed in. There is an adjustment period, and a lot of new users hit a wall in the first few weeks with mask leaks, dry mouth, claustrophobia, or pressure that feels too strong. None of that means CPAP is wrong for you. It usually means a setting needs adjusting or a piece of equipment needs trying. The fix is to stay in contact with your prescriber rather than to quit.
A few things I would tell my pre-diagnosis self
Get the test. Whatever the discomfort or hassle is, it is small compared to years of untreated apnea grinding down your heart, your brain, and your relationships.
Trust your partner if they are telling you something is wrong. They watch you sleep. You do not.
Ask questions about your report. The numbers are yours.
If your first CPAP setting feels wrong, go back. Adjustments are part of the process. Mine had to be lowered before therapy actually felt right.
Common questions
Is a sleep study uncomfortable? The lab version is a little strange the first time. You will be wired up, and you are sleeping in a bed that is not your own. Most people fall asleep faster than they expect to. A home test is far less intrusive, though older systems with multiple cables and a chest belt take some getting used to.
What if I cannot sleep during the test? Labs only need a few hours of usable data, and you usually sleep more than you think. If a lab night truly does not produce enough data, the study can be repeated.
Can I bring my own pillow and pajamas? Yes, and it helps. Familiar items make the room feel less clinical.
Will I need CPAP forever? Not always. Some people improve significantly with weight loss, surgery, or oral appliance therapy. For many of us, CPAP is the safest and most effective long term option, but treatment plans can change over time.
Does insurance cover a sleep study? In most cases yes, when the study is ordered by a doctor and meets the insurer’s criteria. Coverage details vary by plan, country, and provider, so the only honest answer is to check with your own insurer before the test.
A final word
A CPAP sleep study sounds intimidating from the outside, especially the in lab version with its sensors and wires. The reality is that it is one of the more useful nights you can spend in your own life if you have been waking up tired for years and do not know why. It produces a number, the AHI, that translates almost directly into a treatment plan. From there, the work shifts from diagnosis to dialing in therapy, and that is where the actual recovery happens.
If you are still on the fence, talk to your doctor. The conversation is free. The test, in either form, is finite. What is on the other side, in my experience, is a different way of feeling in your own body.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).