Troubleshooting CPAP Problems: From a 12+ CPAP User

Three weeks into CPAP therapy, back in 2014, I woke up at quarter past two in the morning to a noise I couldn’t place. A thin, high-pitched hiss. My mouth felt like I’d been chewing on a sponge and left it out in the sun. The mask had shifted about half an inch down my face while I slept, and the escaping air was blowing directly into my left eye. I lay there for a good thirty seconds trying to work out whether I was awake or having a particularly detailed stress dream. Then I seriously, genuinely considered picking up the whole machine and walking it out to the wheelie bin.
I didn’t, obviously. I’m writing this twelve years later, still using CPAP every night, still sleeping better than I did for most of my adult life before it. But that moment at two in the morning is the reason this post exists. Because what nobody really tells you when you get diagnosed with sleep apnea and handed a CPAP machine is that the first few weeks are almost entirely a troubleshooting exercise. The therapy itself is extraordinarily straightforward, the hardware is reliable, and the science is settled. It’s the fit, the feel, the settings, and the small, stupid problems that you have to beat one at a time.
I’ve been using the same ResMed AirSense 10 for most of the last decade (a few masks have come and gone). In that time I’ve dealt with mask leaks serious enough to wake the neighbours, dry mouth that didn’t respond to anything for two months, rainout that soaked my pillow, aerophagia that made me genuinely anxious about eating dinner, a cracked humidifier chamber, EPR settings I’d accidentally turned off for six months without noticing, and a filter I let go so long it started whistling. If there’s a common CPAP problem I haven’t had, I probably just haven’t had it yet.
Here’s what I want you to take from this post: virtually every common CPAP problem has a fix, and most of those fixes are cheaper, simpler, and less dramatic than you’d expect. You just need to know what you’re looking for. Mayo Clinic’s troubleshooting guide covers the same ground from a clinical angle, and I’d recommend reading it alongside this post if you want the full picture. Everything below is how it’s played out in my own bedroom, with my own face, over a long enough time that I’ve probably tried the wrong fix before finding the right one.
Why CPAP Problems Happen in the First Place
Most CPAP issues aren’t machine problems. They’re interface problems. The machine itself is basically a small, quiet, extremely reliable fan attached to a humidifier. It runs for ten thousand-plus hours without drama. What changes night to night is everything around it: your face, your position, the room temperature, the humidity, whether you’ve had a cold, whether your mask cushion has aged another week, whether the hose has a micro-tear you can’t see.
Knowing that up front helps, because it stops you blaming the machine for things the machine isn’t doing. Nine times out of ten the problem is the mask. The rest of the time it’s usually the humidifier setup, the pressure, or something you can’t see on the filter.

Mask Leaks
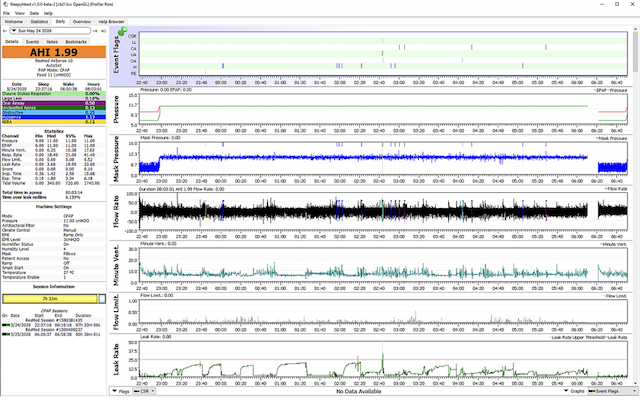
This is the big one. Mask leaks are probably the most universal CPAP complaint and they’re where I’d start if anything about your therapy feels off. A leak makes noise that will wake you or your partner, reduces how effective your therapy actually is (your AHI number on the app the next morning is the giveaway), and if the escaping air is blowing toward your face, it’ll dry your eyes out and make the whole experience miserable.
The counterintuitive thing I learned within my first few months is that tightening your straps usually makes leaks worse rather than better. That was the first trap I fell into. My mask started leaking about eight weeks in and my instinct was to clamp the headgear down as hard as I could, as if I was trying to seal a dodgy pressure cooker. What that actually does is distort the cushion against your skin, which breaks the seal in a different place. It looks tighter but it seals worse.
What fixed it was replacing the cushion entirely. Face oils and skin cells break down silicone faster than most people realise. A cushion can look completely fine to the eye and still have lost enough of its integrity to stop sealing properly. I replace mine every two to three months now and I calendar it, because otherwise I forget. If you’ve never replaced a cushion, that’s probably step one.
The second trick is fitting your mask while lying down in your actual sleeping position rather than sitting upright in front of a mirror. A seal that looks perfect when you’re upright can open up the moment you roll onto your side or your stomach. I’m a side sleeper, and the amount of leak I was getting when my cheek pressed into the pillow took me embarrassingly long to diagnose, because every time I checked in the bathroom mirror the seal was fine.
Mask liners helped enormously once I started using them. These are thin fabric inserts that sit between your skin and the cushion — they soak up oils, improve the seal, and stopped the skin irritation I was getting around the bridge of my nose. My breakdown of the best CPAP mask liners covers the ones I’ve actually tried.
If you’ve done all of that and you’re still leaking, the mask style itself might just not suit your face. That was eventually the conclusion I came to after fighting a particular full-face model for months. Narrow nose bridges, wide cheekbones, beards, glasses, and jaw shape all change what works. My full write-up on why CPAP masks leak goes deeper on mask geometry if you want to keep digging.
Dry Mouth and the Mouth-Breathing Problem
Waking up with a mouth like sandpaper was my longest-running CPAP problem, and for a long time I couldn’t work out why. I was using a nasal mask at the time. Turns out I’m a mouth breather, and when you’re a mouth breather wearing a nasal mask, the pressurised air enters through your nose and exits through your open mouth all night long. Your mouth becomes a wind tunnel. The effect is exactly as miserable as it sounds and no amount of humidification fully solves it, because you’re essentially running a hair dryer through your face for seven hours.
The most direct fix if you’re in this situation is switching to a full face mask. That’s what I eventually did, and the difference was immediate. There was a brief adjustment period where the larger mask felt more intrusive, but the dry mouth disappeared within a night. My comparison of nasal vs full face CPAP masks covers the trade-offs properly.
The other option, if you prefer nasal masks or pillows, is a chin strap. These hold your mouth closed while you sleep so the air can’t escape. I tried one for about six weeks before giving up and switching mask types — they work for some people but I found the strap itself more uncomfortable than just changing mask, and I never quite trusted that my mouth was staying closed. The best CPAP chin straps post covers the ones worth considering if you want to try this route before committing to a new mask.
The third piece of the dry-mouth puzzle is the humidifier, and this was the one I got wrong for an embarrassingly long time. Modern CPAP machines have a heated humidifier built in, but for my first year I had mine cranked way too low because nobody had explained to me how it actually worked. Turning it up properly, combined with heated tubing, made a bigger difference to my comfort than almost any other change I’ve made. My full guide on CPAP dry mouth has the step-by-step I wish I’d had.
Rainout and Condensation

If you’ve ever been woken up by water droplets hitting you in the face through your mask, or gurgling noises coming out of your hose at three in the morning, congratulations — you’ve met rainout. It’s one of the ruder awakenings CPAP has to offer.
What’s happening is physics. The humidified air leaving your machine is warm. As it travels through the hose, particularly if your bedroom is cooler than the air coming out of the machine, the temperature drops and the moisture condenses. Instead of a nice humid breath, you get actual water droplets pooling in the hose and then either gurgling back toward the machine or being blown straight at your face.
The most effective fix is heated tubing, which keeps the hose itself at a consistent temperature so the moisture stays as vapour. My ResMed has this built in and it effectively eliminated my rainout years ago. If your machine doesn’t have heated tubing, an insulated hose cover works reasonably well as a stopgap. You can also turn your humidity setting down a couple of notches, though for me that traded rainout for dry mouth, which wasn’t an improvement.
One other thing worth checking: where you’re putting the machine relative to the bed. If the machine sits higher than your head, water that does condense drains toward your face. If it sits lower, it drains back toward the machine and collects harmlessly in the humidifier chamber. I keep mine on a low bedside shelf specifically for this reason. There’s a detailed walkthrough in my CPAP rainout guide if condensation is your main battle right now.
Pressure That Feels Wrong
If breathing against your CPAP feels like a fight — whether that’s struggling to exhale or feeling like you’re not getting enough air in — the settings are almost always adjustable. One thing I’ll say firmly before going further: don’t change your prescribed pressure without talking to your doctor or sleep tech. That number came from your titration study and the AHI data they collected. Mess with it and you might be treating your apnea less effectively, which is the whole point of being on CPAP in the first place.
What you can adjust yourself on most machines is the ramp function. Ramp starts the machine at a lower pressure and builds it up gradually over the first fifteen to thirty minutes while you fall asleep. I use it every single night. Going from quiet room to full prescribed pressure in a single second is jarring in a way that ramp completely solves. On the ResMed AirSense series, it’s in the comfort settings menu and you can set both the starting pressure and the ramp duration.
The other setting worth knowing about is EPR, which stands for Expiratory Pressure Relief. EPR drops your pressure slightly during exhalation, so it feels less like you’re breathing out against a wall. It comes in levels from 1 to 3. I’ve had mine on 3 for years. Philips machines call their version Flex. Both do the same thing. If exhalation feels laboured, this is the first setting to look at.
For a deeper dive into what each number on your app actually means, my post on CPAP pressure settings goes into it without getting lost in the jargon. And if you’re curious about reading your overnight data properly, interpreting CPAP data is a good starting point.
Swallowing Air (Aerophagia)
This one took me a while to identify because it doesn’t feel like a CPAP problem at first — it feels like something you ate. You wake up bloated, gassy, uncomfortable, with a full belly and no particular idea why. I spent about a month blaming dinner before I connected the dots.
What’s happening is that during sleep your throat muscles relax, and at higher pressure settings the air can travel down your oesophagus instead of (or as well as) your lungs. It tends to be worse when you sleep on your back, because the geometry of your throat and oesophagus line up in a way that makes the problem more likely.
The fix that helped me most was boringly simple: change sleep position. Moving from back-sleeping to side-sleeping cut the problem almost in half within a week. I started using a body pillow to stop myself rolling onto my back during the night, which was probably worth more than any setting change.
If position changes don’t help and the bloating is persistent and genuinely disruptive, talk to your sleep specialist. In some cases, switching from CPAP to a BiPAP (which uses two different pressures — one for breathing in, a lower one for breathing out) reduces the total pressure load and takes aerophagia off the table. I wrote more about this in my piece on why CPAP makes me burp, which sounds like a faintly embarrassing blog title but answers a question a lot of people quietly Google at four in the morning.
Noise From the Machine or Mask
A well-functioning CPAP machine should be almost silent. If yours is suddenly louder than you remember, something has changed. The filter is usually the first thing to check. Disposable filters clog with dust, skin flakes, and pet hair faster than you’d expect, and a clogged filter forces the motor to work noticeably harder. I replace disposables every couple of weeks and wash the reusable ones whenever I’m doing a weekly clean.
Other common noise sources:
A whistling sound almost always means a mask leak. The vent holes on a CPAP mask are designed to release exhaled CO₂, but if the mask seal has broken somewhere else, the air whistles through the gap. Re-seat the mask, check the cushion.
Gurgling means rainout. See above.
Vibration against a hard surface is the sneaky one. I spent a week thinking my machine was dying before I worked out it was just resonating against my wooden bedside table. A folded hand towel under it, or a silicone anti-vibration mat, dampens it completely.
Loose hose connections at the machine, humidifier, or mask end will also buzz quietly. Twist each joint firmly.
If you’ve done all of that and the motor itself still sounds wrong — a grinding, whining, or intermittent tone — it may be at the end of its natural life. My guide on how long a CPAP machine lasts covers the warning signs.
Claustrophobia and Anxiety
This one doesn’t get talked about enough and it was a bigger problem for me, in the first fortnight, than any of the physical issues. Wearing a tight mask strapped to your face in the dark is a strange sensation for almost everyone, and for some people it’s genuinely distressing. I’ve seen people on CPAP forums describe ripping their masks off in their sleep repeatedly without waking — which is your subconscious brain making an extremely clear statement about how it feels about the situation.
The thing that worked for me was graduated exposure during the day. Not at bedtime. Wearing the mask while watching TV in the evening, with the machine running at ramp pressure, lets your nervous system start pairing the mask with neutral or even pleasant experiences rather than bedtime stress. By the time you put it on at night, the sensation is familiar rather than foreign.
Starting with a less intrusive mask helps too. Nasal pillows are the smallest and least claustrophobic option, and some people find it worth starting there even if they’ll eventually move to a different mask style. If full face masks trigger claustrophobia hard, you don’t have to start there.
The third thing, and I nearly didn’t put this in because it sounds obvious: don’t try to fight through it alone if it’s not getting better. Sleep psychologists work specifically on CPAP anxiety and they do in a few sessions what most of us wouldn’t achieve in a year of solo trial and error. Sleep Foundation’s guide on getting used to CPAP has a good overview of the desensitisation approach. My longer post on overcoming CPAP anxiety covers what worked for me specifically.
Stuffy or Runny Nose
This one isn’t on everyone’s list but it’s extremely common and it caught me off guard in winter. Pressurised air blowing through your nose all night can irritate the nasal membranes, especially if your humidity is too low or you’re already fighting mild allergies. The result is either a persistent runny nose in the morning or, paradoxically, a completely blocked one.
The first fix is humidity. A dry nasal passage is an irritated nasal passage. If your humidifier is running cool or low, turn it up a notch and see what happens over a week. The second fix, which I still do on and off, is a saline nasal rinse before bed. Not a decongestant — those create rebound congestion and make things worse over time — just plain saline. It clears the pathway and reduces morning stuffiness considerably.
If you suspect allergies are part of the picture, a high-quality hypoallergenic filter for your machine is worth trying. ResMed and Philips both make them; they fit the same slot as the standard disposable filter but catch finer particles.
And if you’re genuinely sick with a cold or sinus infection, my guide on using CPAP when sick covers what to change (and what not to change) during the illness.
Red Marks, Skin Irritation, and Dermatitis

Yep, this is me.
If you’re waking up with deep pressure marks across your cheeks or the bridge of your nose, something isn’t right. A well-fitted mask should leave faint impressions at worst. Deep marks that stay for half an hour or more mean the mask is too tight or the cushion is sitting against the wrong part of your face.
Loosen the straps first. Most people, myself included, initially over-tighten the mask to prevent leaks. Start with the straps almost loose, turn the machine on, and only tighten until the leaks stop. You should be able to slip a finger under the strap.
If the cushion is leaving indentations regardless of strap tension, the cushion itself might be the wrong size or shape. Many mask lines come in S/M/L cushions and the sizing isn’t always obvious at the chemist. I wore a medium for nearly two years before discovering I should’ve been on a small the whole time.
For genuine skin irritation — redness that doesn’t fade, acne-like breakouts under the mask, or patches of eczema — the issue is usually trapped oil and bacteria. Cleaning the cushion daily with a gentle fragrance-free wash usually solves it. In persistent cases, what you’re dealing with is CPAP dermatitis, which has its own dedicated fixes. My post on preventing CPAP mask lines covers the cosmetic side if you’re self-conscious about the morning marks.
A related issue is CPAP dry eyes, which is usually caused by a micro-leak near the top of the mask, blowing air up into your eye sockets all night. If you’re waking up with gritty, irritated eyes, check the seal at the bridge of your nose first.
Data Sync, Error Messages, and the App That Won’t Talk to Your Machine
Modern CPAP machines phone home to apps like myAir (ResMed) or DreamMapper (Philips). When they stop doing it, people assume the machine has broken, which it almost never has.
The first thing to check is whether Airplane Mode is on. On ResMed AirSense machines it’s a small aeroplane icon that appears in the top corner when toggled, and it turns off all wireless comms. I flicked mine on by accident during a hotel stay in 2022 and spent three days wondering why my data had vanished.
The second thing is Bluetooth pairing. Open the app, remove the device, and re-pair from scratch. This solves maybe seventy per cent of sync failures.
If you use your machine in a poor-signal area — a basement bedroom, a house with thick brick walls, a rural area — cellular-based machines may struggle. In that case, connecting the machine to Wi-Fi (if your model supports it) is often more reliable than cellular.
For error codes specifically, check your machine’s manual or the manufacturer app first. Most error codes point to something simple: filter replacement due, humidifier not seated properly, hose not connected. If you want to go deeper into your therapy data than the consumer apps show you, OSCAR software lets you pull the SD card out of the machine and see everything the manufacturer’s app smooths over.
Keeping On Top of Maintenance
Most CPAP problems I’ve had across a decade trace back to equipment that needed cleaning or replacing. The maintenance isn’t complicated, but it does need consistency.
I rinse my mask cushion with warm water every morning. I do a proper soapy wash of the mask, headgear, and hose every week. I clean the humidifier chamber at the same time. Once a month the chamber gets a vinegar soak to deal with any mineral build-up. My full walkthrough of how to clean a CPAP machine has the exact routine if you want something to follow.
Replacement schedules matter as much as cleaning, and they’re the thing people ignore most. Mask cushions every one to three months. Headgear straps every six months or so — they stretch and lose tension and then your mask slips even though nothing else has changed. Hoses develop micro-cracks over time that you can’t always see but that show up as mystery leaks and inconsistent pressure. Filters every two to four weeks for disposables, weekly rinses for reusables. The full rundown is in my CPAP replacement schedule, and following it has eliminated about ninety per cent of the troubleshooting I used to do.
One more thing on maintenance, and I know I sound like a broken record on this: always use distilled water in your humidifier. Tap water leaves mineral deposits that are hard to clean out and eventually affect how the humidifier performs. A two-litre bottle costs a couple of dollars and lasts me a fortnight.
When to Get the Machine Itself Checked
Most CPAP machines last five to seven years with normal care. Problems during that time almost always come from parts wearing out rather than the machine failing. But if you’re getting repeated error messages you can’t resolve, the motor is making noise even with a fresh filter, or the machine is consistently struggling to hold your prescribed pressure (you’ll see this as widely varying pressure numbers on the app), it might be signalling something structural.
Warranties vary by machine and region. Mine was two years on the unit itself and the humidifier, with shorter terms on the hose and filters. If you’re still in warranty and the machine is acting strangely, take it back to your supplier before you replace any part of it. If you’re out of warranty, it may be cheaper to upgrade than repair, especially as newer models have better humidifiers, quieter motors, and smarter data.
Frequently Asked Questions
How long does it take to get used to CPAP?
Most people adjust within two to four weeks. Some take three months. Very few take longer, and those who do usually benefit from switching masks or seeing a sleep psychologist. My post on getting used to CPAP therapy walks through the typical adjustment curve.
Is it normal to take off my mask in my sleep?
It’s common in the first few weeks, especially if you’re dealing with leaks or claustrophobia. If it continues past a month, the mask or the pressure probably needs adjusting — it’s not just willpower.
Should I stop using CPAP if I have a cold?
No, generally. Keep using it but turn up the humidity, consider a saline rinse before bed, and use a clean filter. Full details in my guide on using CPAP when sick.
Can I travel with a CPAP machine?
Yes. Most modern machines are TSA-approved and don’t count toward your carry-on limit. A travel CPAP is worth considering for frequent trips. My guide on the best way to travel with CPAP covers batteries, adaptors, and airport procedures.
How do I know if my therapy is actually working?
Check your AHI number on the app each morning. Under 5 events per hour is the treated range. If you’re above 5 regularly, either the pressure, the mask seal, or both need adjustment, and it’s worth booking a follow-up with your sleep doctor.
The Honest Truth About Sticking With It
The early weeks of CPAP therapy have a way of making you question whether it’s worth the trouble. The mask, the straps, the noise, the dryness, the pressure, the leaks, the bloating, the dreams where you keep pulling it off. It’s a lot to adjust to all at once, and it’s legitimately harder than anyone warned me it would be.
But the other side of that adjustment is real, and it’s the reason I’ve kept going for more than a decade. Before CPAP, my AHI was in the severe range — I was stopping breathing dozens of times an hour, every hour, every night. I was falling asleep at traffic lights. I was angry all the time in a way I couldn’t explain. The difference between that version of me and the one typing this sentence is enormous, and it’s entirely down to a small fan blowing pressurised air through a piece of silicone against my face.
Almost every problem I’ve described in this post has a practical fix. The fixes are usually simpler than they seem at two in the morning when nothing is working. If you’re in the troubleshooting phase right now, keep going. The right combination of equipment and settings is out there, and once you land on it, you mostly stop thinking about it at all. That’s the goal. That’s what it looks like on the other side.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).