Hypothyroidism and Sleep Apnea: What the Connection Means

Let’s get real. My background is in computer science, not medicine, and I have never had a thyroid problem myself. What I do have is more than a decade of living with severe obstructive sleep apnea and a long habit of reading the research closely so I understand my own condition. Hypothyroidism is one of those topics that comes up again and again in sleep apnea circles, usually framed as a question: if my thyroid is underactive, is that why I stop breathing at night, and will fixing my thyroid fix the apnea too?
It is a fair question, and the honest answer is more layered than most quick articles admit. So this is a research report, not a personal story. I have pulled together what the medical literature actually says about hypothyroidism and sleep apnea, and I have tried to separate what is well established from what is still uncertain.
A quick refresher on what each condition is
Hypothyroidism means the thyroid gland, the small butterfly-shaped gland at the front of your neck, is not making enough thyroid hormone. Those hormones set the pace for a huge range of body functions, from heart rate to body temperature to how quickly you burn energy. When levels drop, everything tends to slow down. The classic signs are fatigue, weight gain, feeling cold, dry skin, low mood, and a kind of mental fog.
Sleep apnea is a breathing disorder. In the obstructive form, the muscles and soft tissue at the back of the throat relax during sleep and block the airway, so breathing pauses again and again through the night. If you want the full picture of the condition, I cover it in detail in what is sleep apnea. The point worth holding onto here is that obstructive sleep apnea is mechanical. Something is physically narrowing or collapsing the airway.
That mechanical reality is exactly where the thyroid enters the story.
Why an underactive thyroid raises sleep apnea risk
The link between hypothyroidism and sleep apnea is not folklore. Researchers have been documenting it since at least the 1980s, and analyses of large US health survey data have found that people with hypothyroidism are more likely to also carry a sleep apnea diagnosis. The relationship is not as simple as one causing the other in a straight line, but there are several plausible ways an underactive thyroid can make the airway more prone to collapse.
The first is tissue thickening. Long standing low thyroid function can lead to deposits of proteins and complex sugars in the soft tissues of the body, including the tissues lining the upper airway. The throat effectively becomes a little bulkier and a little less springy, which leaves less room for air to pass and makes the airway easier to obstruct once the muscles relax in sleep.
The second is enlargement of nearby structures. Hypothyroidism is associated with an enlarged tongue, and in some people the thyroid gland itself swells into a goiter that sits right at the base of the windpipe. Either change crowds the same narrow space that air has to travel through.
The third is weight. Because thyroid hormone governs metabolism, an underactive thyroid commonly leads to weight gain, and extra weight around the neck and throat is one of the strongest contributors to obstructive sleep apnea. This is one of the few places where the two conditions feed each other in a way you can act on, and it is part of why managing weight matters so much for breathing at night. I go deeper into that relationship in CPAP therapy and weight loss.
The fourth is muscle and nerve signaling. Thyroid hormone affects how muscles work and how nerves carry signals to them. With less of it, the muscles that are supposed to hold the upper airway open can become weaker and slower to respond, so the airway gives way more easily.
The fifth mechanism reaches beyond the throat entirely. Thyroid hormone also influences the brain’s control of breathing, the automatic drive that tells your body to take the next breath. When that drive is blunted, breathing during sleep can become shallow or irregular in a way that looks less like a blocked airway and more like the brain simply not sending the signal. That pattern overlaps with central sleep apnea, which is a different beast from the obstructive kind. If that distinction is new to you, I explain it in central sleep apnea. The takeaway is that hypothyroidism can nudge breathing in more than one direction at once.
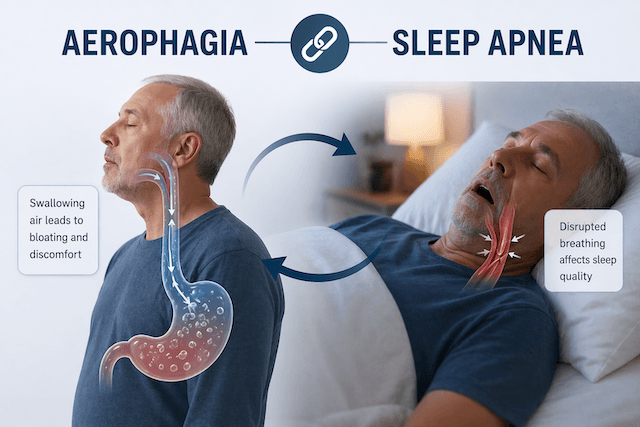
The overlap that makes both conditions easy to miss
Here is the part that I find genuinely tricky, and it is the reason thyroid testing belongs in any good sleep apnea evaluation. The two conditions share almost all of their headline symptoms.
Think about what untreated hypothyroidism feels like: exhausted during the day, foggy, heavy, low. Now think about what untreated sleep apnea feels like: exhausted during the day, foggy, heavy, low. They are nearly identical from the inside. Someone with both can easily have one diagnosed and treated while the other hides in plain sight, because the lingering tiredness gets blamed entirely on the condition already on the chart.
There is a quieter version of this problem too. A meaningful share of people with moderate to severe sleep apnea turn out to have a mild form of hypothyroidism called subclinical hypothyroidism, where thyroid levels are only slightly out of range and the symptoms are too vague to raise alarm. Because it is so easy to overlook, it can sit untreated for a long time. Worth knowing as well is that the degree of thyroid dysfunction does not reliably predict how severe the sleep apnea will be, so a thyroid result that looks only a little off does not rule out a real contribution to your breathing at night.
I know how convincing that daytime exhaustion is, because it was the thing that finally pushed me toward a diagnosis years ago. The full version of that story lives on my sleep apnea symptoms page. What matters for this discussion is that fatigue is a terrible diagnostic clue on its own. It points at too many things. That is exactly why a doctor evaluating you for sleep apnea may order a simple blood test to check your thyroid hormone levels, and why someone newly diagnosed with hypothyroidism who is still wiped out after treatment should ask whether their sleep has ever been properly assessed.
Will treating the thyroid fix the sleep apnea?
This is the question almost everyone really wants answered, and it is where I have to be careful not to oversell.
Sometimes, treating hypothyroidism does improve the apnea. There are documented cases where bringing thyroid levels back to normal with hormone replacement reduced the number of breathing events, and occasionally the improvement is large enough that the sleep apnea no longer needs separate treatment. That outcome is real, and it is most likely when the thyroid problem was a major driver of the airway trouble in the first place.
But it is far from guaranteed. A great deal of the research points the other way. In several follow up studies, people whose thyroid levels were successfully restored still had significant sleep apnea afterward, with breathing events barely changed. Sleep apnea usually has more than one cause working at the same time, things like jaw and airway anatomy, weight, age, and muscle tone, and correcting the thyroid only removes one piece of that. The current expert view is that you should not count on thyroid treatment alone to clear sleep apnea, and you should not delay starting sleep apnea treatment while you wait to see whether your thyroid numbers settle. The breathing disruption is doing damage every night it goes untreated, and that is not worth gambling on a maybe.
There is also a safety angle here that does not get enough attention, and it is important enough that I want to flag it plainly even though I am not a clinician. Starting thyroid hormone replacement asks more of the heart, because it speeds the body’s metabolism back up. In a person who also has untreated sleep apnea, the heart is already under strain from the repeated drops in oxygen overnight. Older clinical reports describe heart rhythm problems and chest pain emerging when thyroid treatment was begun in patients whose sleep apnea had not yet been addressed. This is firmly a conversation to have with your own doctor, but it is a strong argument for treating the two conditions together and under supervision rather than assuming the thyroid medication will quietly take care of everything. The combination of airway support at night and carefully managed thyroid replacement is the approach that shows up repeatedly in the literature.
What this means if you suspect both
If you have hypothyroidism and you are still tired, snoring, waking unrefreshed, or your partner notices you stop breathing, treat that as a reason to get your sleep looked at properly rather than chalking the fatigue up to your thyroid. And if you already know you have sleep apnea, it is reasonable to make sure your thyroid has been checked at least once, since the two travel together often enough that good clinicians screen for it.
Getting assessed is far less of an ordeal than it used to be. My own diagnosis came through a home sleep test, the kind you do in your own bed rather than wired up in a lab overnight, and the technology has only improved since. I walk through the options in at home sleep apnea test. A thyroid check, meanwhile, is a routine blood test your doctor can order alongside everything else. Neither step is dramatic, and together they can explain a lot of misery that people otherwise just learn to live with.
The reassuring part, and I say this as someone who has relied on the therapy for years, is that the main treatment for obstructive sleep apnea works on the airway itself, independent of why the airway is collapsing. A CPAP machine holds the airway open with a gentle stream of pressurized air, so it keeps you breathing whether the underlying contributor is your weight, your anatomy, an underactive thyroid, or some combination. That does not make the thyroid irrelevant, because the metabolic effects of hypothyroidism reach well beyond sleep and deserve their own treatment. It just means the breathing problem has a reliable answer while you and your doctor sort out the rest.
The bottom line on hypothyroidism and sleep apnea
An underactive thyroid is a genuine risk factor for sleep apnea, working through thicker airway tissue, an enlarged tongue or gland, weight gain, weaker airway muscles, and a blunted drive to breathe. The two conditions share so many symptoms that either one can easily hide the other, which is the best reason to make sure both have been checked when the daytime fatigue does not add up.
Treating the thyroid sometimes helps the apnea and sometimes does not, so it is not a substitute for treating the sleep apnea directly, and starting thyroid medication while sleep apnea goes untreated is something to do only with medical guidance. None of this is cause for alarm. Both conditions are common, both are very treatable, and the path forward starts with two fairly ordinary tests and an honest conversation with your doctor.
For a balanced overview of how thyroid activity and sleep interact, the Sleep Foundation is a solid starting point, and the clinical relationship between the two conditions is laid out in this review on the mechanisms and management of sleep apnea in hypothyroidism.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).