Drooling with CPAP: Why It Happens (and How to Finally Stop It)

Waking up to a damp pillow, a soggy mask cushion, or saliva on your face is one of those small CPAP indignities that nobody warns you about. It happens to plenty of CPAP users, and it has happened to me. I notice it more when I am fighting a cold or my sinuses are acting up.
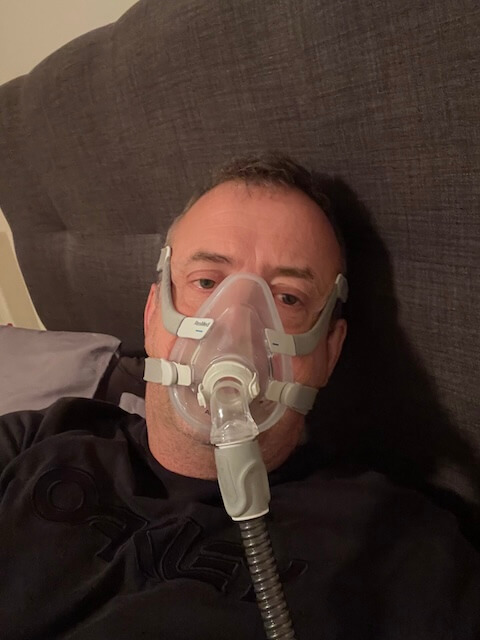
Before I get into the causes and what actually helps, a quick note on my perspective. I have used a CPAP machine for more than a decade for severe obstructive sleep apnea. I am a chronic mouth breather, which is why I have always used a full face mask rather than nasal pillows or a nasal cushion. My experience with drooling is full face mask experience. Where I write about nasal masks below, I am drawing on what other users commonly report and what the available guidance suggests, not on personal trial. Background note while we are at it: my training is in computer science, not medicine, so treat what follows as one patient’s perspective rather than clinical advice.
Drooling is mostly a comfort and hygiene issue, not a sign that your therapy has gone wrong. In some ways it is the opposite. People often report more drool only after they start sleeping deeply on CPAP, because the muscles around the jaw and lips finally relax in a way they had not before treatment. That is not a problem. It is biology meeting a mask. The goal of this guide is to help you understand which version of the problem you have, and what generally works for it.
What is actually happening when you drool on CPAP
Saliva production runs in the background all day and night. It does not stop when you sleep. What changes during sleep is your ability to swallow it efficiently and your ability to keep your lips sealed. In deeper stages of sleep, the muscles in your face, jaw, and tongue lose tone. If your lips part or your jaw drops, gravity does the rest.
Add a CPAP machine into that picture and a few things shift. Pressurized air can either dry the mucous membranes (which sometimes triggers your body to compensate by producing more saliva when you wake) or, with a humidifier, add moisture to the system. Mask design changes where the saliva ends up. With a nasal mask or pillows, drool tends to escape onto the pillow. With a full face mask, it has nowhere to go and pools inside the cushion. Different problem, same root cause.
This is also worth saying clearly: a small amount of overnight saliva on your pillow has been a normal human experience long before CPAP was invented. The reason it feels worse now is that you are sleeping with equipment strapped to your face, and any moisture seems more obvious because of it.
The most common reasons CPAP users drool
There are usually one or two main culprits, sometimes a combination. Working through these is the fastest way to identify what is happening on your nights.
Mouth breathing
This is the biggest one. If you breathe through your mouth while you sleep, your lips are parted, your tongue position changes, and saliva escapes. Many people with sleep apnea are mouth breathers to begin with, often because of nasal anatomy, allergies, or just long term habit. Treating apnea does not automatically retrain that habit. The Sleep Foundation has a useful overview of CPAP side effects that includes mouth breathing and dryness, and it is worth a read if you want the clinical picture.
If mouth breathing is your main issue, that is also why you may have ended up on a full face mask. I have an article on preventing mouth breathing on CPAP and another on nasal versus full face masks that go into more detail.
Deeper sleep, relaxed muscles
Once your apnea is well controlled, you spend more time in deeper stages of sleep. Your face fully relaxes. Your jaw drops. Your lips part. Saliva that you would normally manage automatically in lighter sleep starts escaping. Some users find drooling actually appears or increases after the first few weeks of successful therapy, which can feel counterintuitive. It is not a problem with the machine. It is a sign your sleep is finally going somewhere.
Sleep position
Side and stomach sleeping put gravity in charge. Saliva runs to the lowest point of your mouth and out. Back sleeping tends to keep saliva pooled at the back of the throat where it gets swallowed unconsciously. Position matters, but it is rarely the only cause, and you should not force a position that wrecks the rest of your sleep just to manage drool. My guide to sleep positions for sleep apnea gets into the tradeoffs.
Nasal congestion
If your nose is blocked, you mouth breathe by default. Allergies, a head cold, a deviated septum, or even a dry bedroom can switch you over without you realizing. This is the bucket I most often fall into. When my sinuses are flaring up, my drool nights are noticeably worse. Treating the congestion at the source, with saline rinses, antihistamines if appropriate, or simply getting humidification right, tends to fix the drool problem too.
Humidity settings
Too little humidity dries your mouth and throat, which can prompt extra saliva production once you wake. Too much humidity creates condensation in the hose and mask, sometimes called rainout, which can feel like drool even when it is just water from the system. Tuning your humidifier and using heated tubing if you have it can sort out a surprising amount. There is more on the dry mouth side of this in my CPAP dry mouth guide.
Medications and reflux
Several common medications increase saliva production as a side effect, including some antidepressants, certain reflux medications, and a few blood pressure medications. Reflux itself can also cause excess saliva and a wet mouth at night. If your drooling started after a medication change, or if it comes with heartburn or a sour taste, talk to your doctor or pharmacist before assuming it is the CPAP setup.
How drooling shows up with nasal masks
I have not used a nasal mask, so what follows is from reading and from what other users have shared rather than personal experience. With nasal pillows or a nasal cushion, the mask covers the nose only. The mouth is open to the room. Two things tend to happen when you drool on this setup. First, the saliva escapes onto your pillow because nothing is in its way. You wake up to a wet patch. Second, because your mouth is open, you also lose therapy pressure through it, which is its own problem and usually shows up as a dry mouth on waking and possibly as higher AHI numbers on your machine reports.
Common solutions for this group include a chin strap, a nasal mask combined with mouth tape, or switching to a full face mask. I have a chin strap guide that walks through how they fit. On mouth tape: I have not used it, so I will not pretend to have an opinion. The general advice in the user community is to use a tape that is specifically marketed for mouth taping, never household tape, and to talk it through with your sleep clinician first if you have any concerns.
How drooling shows up with full face masks
This is the territory I actually know. With a full face mask, the cushion seals around both your nose and mouth. When you drool, the saliva does not escape onto your pillow because it has nowhere to go. It pools inside the lower part of the cushion, against your chin or the corners of your mouth. You sometimes wake up to a wet sensation on your chin, a slick feeling at the cushion seal, or a cushion that has lost some of its grip because the silicone is wet. In the morning, the mask itself tends to need a more thorough wipe down than it would on a dry night.
The tradeoff is real. The full face mask solves the mouth breathing and air leak problem, which is exactly why it works for me. It does not, on its own, fix drool. It just changes where the drool ends up.
A few things have helped me on the full face mask side specifically. The first is mask liners. A soft fabric liner sits between your face and the cushion and absorbs moisture before it pools. It also reduces leak and skin irritation, which is a useful side benefit. My mask liner guide covers the options. The second is paying attention to mask fit. A mask that is too tight can actually push your jaw open at the sides, which makes the inside of the mask wetter, not drier. If you are constantly cranking the headgear, that is worth looking at. My piece on mask leaks goes into how to find a fit that seals without crushing. The third is daily cleaning. With a full face mask and any drool tendency at all, a quick wipe down in the morning and a proper wash a few times a week is not optional. It also keeps the cushion lasting longer. My cleaning guide covers the routines that have worked for me.
If you want the deeper review of the specific mask I use, I have written one up in my ResMed AirFit F20 review.
What actually helps
Pulling the practical points together, here is the order I would work through if I was starting fresh.
Start with the obvious. Treat any congestion. Check that your humidifier is dialed in for your bedroom climate, not too dry, not pumping out so much moisture that you get rainout. Look at your sleep position. If you are a hard side sleeper, a CPAP friendly pillow can help with both leak and drool by keeping your head supported in a position that works with the mask. There is also a guide to masks for side sleepers if you want to go further down that path.
Then look at the equipment side. If you are on a nasal mask and the drool is bad, a chin strap is a cheap thing to try before you change masks. If you are on a full face mask, mask liners are the single highest leverage thing in my experience. Check your mask is not overtightened. If none of that helps, it may be worth looking at the mask itself, which is what my full CPAP mask guide is there for.
Then look at your inputs. Has anything changed in your medications or your reflux? Have you been more congested than usual? Has your bedroom changed, with new heating or cooling? These are the boring questions, but they often turn up the real cause.
If you have worked through all of that and the drooling is still disrupting your sleep, that is the point at which I would talk to your clinician or sleep specialist. There are medical causes of excessive saliva production that have nothing to do with CPAP, and they are worth ruling in or out.
When drooling is worth taking seriously
Most CPAP drool is annoying but harmless. There are a few situations where it is worth flagging to a doctor. Sudden new drooling that you have never had before, drooling that comes with difficulty swallowing or new facial weakness, drooling alongside heartburn or reflux symptoms, drooling that started after a medication change. Those are not CPAP problems. Those are body problems that happen to be showing up at night because that is when the body is most relaxed.
I am not a clinician, so I will keep this part short. If something feels off beyond the usual cosmetic nuisance of a wet pillow, mention it at your next appointment. CPAP users sometimes assume every nighttime symptom is the machine’s fault. It often is not.
Final thoughts
A bit of drool on the pillow, or inside the mask cushion, is something most CPAP users deal with at some point. It does not mean your therapy is failing. In a lot of cases, it is the opposite: it is the byproduct of finally sleeping the way you are supposed to sleep. The version that matters is the version that is interrupting your nights or making you dread putting the mask on. That version is almost always fixable, usually with a combination of treating any congestion, getting your humidity tuned, and adding a mask liner if you are on a full face setup.
If you have found something that worked for you, please leave a comment. The CPAP community runs on shared notes more than any official guidance, and what works for one person often turns out to work for someone else who has been trying everything.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).