What Is Drug-Induced Sleep Endoscopy (DISE)?
If you have spent any time in waiting rooms or sleep apnea forums lately, you have probably run into the term drug-induced sleep endoscopy. It usually comes up at a specific moment: when CPAP has not worked out, or when a surgeon starts talking about Inspire or another procedure. People hear “endoscopy” and “sedation” in the same sentence and reasonably want to know what they are being signed up for.
I want to be upfront before going any further. My background is in computer science, not medicine, and I have not had this procedure. I have managed my own severe obstructive sleep apnea with CPAP for more than a decade, so I have never gone down the surgical road that drug induced sleep endoscopy is part of. What follows is a patient friendly explanation built from medical literature and the published descriptions of the surgeons who actually perform it. Think of this as one patient reading the research and translating it, not a clinician giving advice.
The problem DISE is trying to solve
Sleep apnea is, at its core, a plumbing problem. During sleep, the soft tissues of the throat relax, and in some people they relax enough to narrow or close the airway. But here is the catch that makes treatment harder than it sounds: the airway does not collapse in the same place or the same way for everyone. One person might close off mainly behind the soft palate. Another might have the base of the tongue falling back. Plenty of people have more than one spot giving way at once.
CPAP sidesteps this question entirely. Air pressure splints the whole airway open, so it does not much matter where the weak point is. That is part of why pressure therapy is the first line treatment and why I have stuck with it. The trouble starts when someone cannot tolerate the machine, or wants an alternative, and surgery enters the conversation. Surgery is local. A procedure that fixes the soft palate does nothing for a tongue that is the real culprit. So the surgeon needs to know, specifically, where the collapse is happening before cutting anything.
You cannot get that answer from an awake examination in a clinic chair. When you are sitting up and conscious, your throat muscles have tone that vanishes the moment you fall asleep. Studies comparing the airway in wakefulness against the airway during sleep have found only modest agreement between the two pictures. A polysomnogram, the overnight sleep study most of us did to get diagnosed, tells you how badly you stop breathing and how often. It does not show the surgeon the anatomy giving way. That gap is exactly what drug-induced sleep endoscopy was invented to fill.
What the procedure actually is
Drug-induced sleep endoscopy, almost always shortened to DISE, is a way of looking directly at the upper airway while a patient is in a sleep-like state. The technique was first described in 1991, and over the years since it has become a standard part of the surgical workup for sleep apnea.
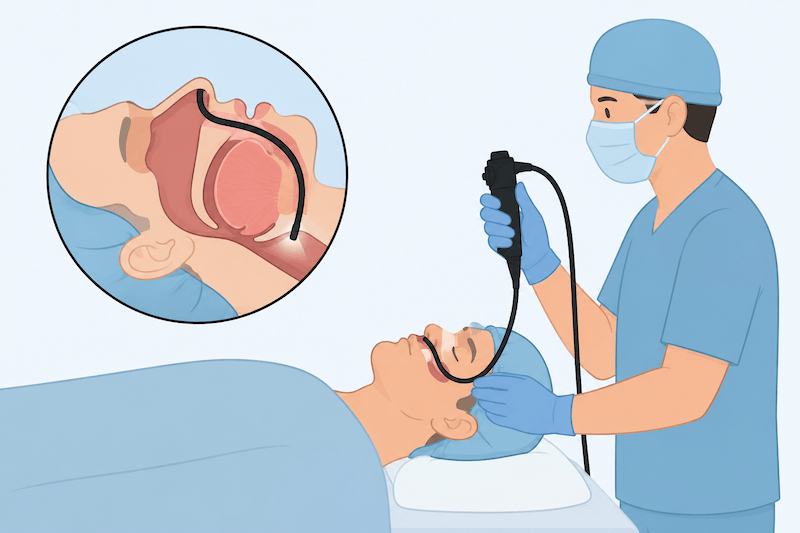
The mechanics are reasonably simple to describe. In an operating room or procedure suite, an anesthetist gives a sedating medication, usually propofol, sometimes with midazolam, to bring the patient into light sleep. This is not general anesthesia. The goal is a depth of sedation that mimics natural sleep closely enough for the throat to behave the way it does at home in bed. Once the patient is under and the tissues have relaxed, a surgeon passes a flexible endoscope, a thin tube with a light and a camera on the end, through the nose and down into the throat.
From there it becomes an observation exercise. The surgeon watches the airway in real time as breathing happens, looking for where and how it narrows or closes. The whole thing is short, often around ten to fifteen minutes of actual viewing, and the patient is woken and moved to recovery afterward. It is typically done as a day procedure, with a period of monitoring before you go home.
There is a variation worth knowing about, sometimes written as DISE-PAP. In that version the surgeon applies gentle CPAP through a mask during the procedure to measure the pressure at which the airway pops open. That can help fine tune a pressure prescription or clarify how the airway responds to support, which is useful information when someone is on the fence between persisting with a machine and pursuing something else.
How surgeons describe what they see
If your surgeon mentions a “VOTE score” afterward, this is what they mean. VOTE is the most widely used system for recording DISE findings, introduced in 2011, and the letters stand for the four anatomical areas the surgeon checks: the velum, which is the soft palate region; the oropharynx, meaning the side walls of the throat; the tongue base; and the epiglottis, the flap of cartilage at the entrance to the voice box.
At each of these four sites, the surgeon notes two things. First, the degree of collapse, usually graded as none, partial, or complete. Second, the pattern, meaning the direction the tissue moves as it closes. The airway can pinch front to back, side to side, or concentrically, like a drawstring bag cinching shut all the way around. That pattern matters more than it might sound. A concentric collapse at the palate, for instance, is generally considered a poor fit for hypoglossal nerve stimulation, which is one of the main reasons the procedure is required before an Inspire implant in the first place.
Surgeons sometimes add a maneuver during the procedure where they gently push the lower jaw forward. If sliding the jaw forward opens the airway, that is a hint that a mandibular advancement device, the kind of oral appliance a dentist fits, might help, since it does the same thing mechanically every night. It is a low cost preview of whether a specific treatment is likely to pay off.
One finding that turns up again and again in DISE research is multilevel obstruction. A large share of patients do not have a single tidy point of collapse. They have two or three areas giving way together, which is sobering if you were hoping for one simple fix, but it is far better to know that going in than to have a single site operation fail because it only addressed part of the problem.
When DISE is on the table, and when it is not
This is the part I think gets lost in the anxiety. You do not get a drug-induced sleep endoscopy when you are first diagnosed. It is not a screening test and it will not tell you whether you have sleep apnea. By the time DISE is being discussed, you have already been diagnosed, and the conversation has moved on to what to do about it.
In practice, the procedure tends to come up for a few overlapping groups. There are people with mild or moderate apnea who would rather pursue a targeted fix than commit to nightly pressure therapy. There are people with more severe apnea who have genuinely tried CPAP and could not make it work, whether because of tolerance issues, mask problems, or pressure they could not get used to. And there are people specifically being evaluated for nerve stimulation, where the procedure is essentially mandatory to confirm candidacy.
What unites all of them is that surgery or a device is already a realistic option they are willing to consider. There is little point looking at the precise architecture of someone’s airway collapse if they have no intention of acting on what is found. That is why the literature frames DISE as a tool for selecting alternatives to CPAP rather than as a routine diagnostic.
It is also why I have never had one. Pressure therapy worked for me, I tolerate my full face mask well as a chronic mouth breather, and so the question of where exactly my airway collapses has never needed answering. Plenty of people are in the same boat. If CPAP is doing its job, this procedure is not part of your story, and that is a good thing.
What the procedure can and cannot promise
It would be easy to read all this and assume DISE guarantees a successful surgery. It does not, and the honest picture from the research is more measured. Studies looking at whether a DISE guided plan improves surgical outcomes have produced mixed results, though the overall weight of evidence leans toward it being more informative than the cheaper, less invasive awake assessments it competes with. One frequently cited observation is that the findings change the proposed surgical plan in roughly half of cases, which tells you the procedure is genuinely adding information rather than rubber stamping a decision already made.
What DISE does well is map the territory. It shows the surgeon where the airway fails and how, and it lets them tailor a procedure to that specific anatomy instead of guessing. Whether the chosen procedure then succeeds depends on many other things, including how many sites are involved, the patient’s weight, and how the body heals. A good map improves your odds. It does not move the destination guarantee into the certain column.
It is also worth being clear-eyed that this is a sedated procedure, and sedation carries its own considerations. People with certain medical risk profiles, allergies to the sedating drugs, or central sleep apnea rather than the obstructive kind may not be suitable candidates. Those calls belong to the anesthetist and surgeon, who weigh them against your full history. This is not a procedure you talk your way into casually.
Where it fits alongside everything else
I find it helps to picture the sleep apnea toolkit as a sequence rather than a menu. Diagnosis comes first, usually through a sleep study. CPAP is offered as the standard treatment because it works regardless of where the collapse is. For people who cannot or will not use pressure therapy, the question shifts to alternatives, and that is where the airway’s specific anatomy suddenly matters a great deal. Drug induced sleep endoscopy is the step that supplies that anatomical detail, feeding into decisions about oral appliances, nerve stimulation, soft palate operations like uvulopalatopharyngoplasty, or even simpler measures. Some DISE protocols also test airway behavior with the head and trunk elevated, which can flag a strong positional component worth addressing before anything more invasive.
Seen that way, DISE is not a treatment at all. It is a decision making tool, and a fairly precise one, that sits between deciding to leave CPAP behind and choosing what comes next. If you are being offered it, that is usually a sign your care has reached the point of taking alternatives seriously, which can feel daunting but also means someone is trying to match the fix to your actual anatomy rather than handing you a generic one.
For readers who want the clinical view from the surgeons who perform it, the explainers from Mount Sinai and UChicago Medicine are both readable and grounded in actual practice. They are the kind of sources I would want my own family reading if this procedure ever came up for them.
The short version
Drug-induced sleep endoscopy lets a surgeon watch your airway collapse under sleep-like sedation, so they can see exactly where and how it fails before recommending a procedure. It is not a diagnostic test, it is not something you encounter early, and it is not a promise that surgery will work. It is a way of replacing guesswork with a clear picture, reserved for the moment when you and your doctor are seriously weighing an alternative to CPAP. If pressure therapy is keeping your numbers down, this is one corner of the sleep apnea world you can happily leave unexplored.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).