Sleep Apnea and Sex: The Connection and Help

Ask anyone who has been on CPAP therapy for any length of time and a version of the same conversation eventually comes up. Often quietly. Usually not on the first appointment. Sleep apnea changes more than your nights. It affects energy, mood, attention, and yes, sex.
I’ve been on CPAP for more than a decade since being diagnosed with severe obstructive sleep apnea. I’m not a doctor. My background is in computer science, not medicine. But after years of reading patient forums, listening to people in CPAP communities, and living with the therapy myself, this is one of the topics that comes up far more often than most clinicians realize. People are embarrassed to raise it with their sleep specialist. They Google instead. So let’s talk about it honestly.
What the research actually shows The link between sleep apnea and sexual health is not folklore. It is one of the more consistently documented hidden effects of untreated OSA, and the underlying mechanisms are no longer mysterious.
The American Academy of Sleep Medicine reported on a study from Walter Reed National Military Medical Center that followed 92 men newly diagnosed with obstructive sleep apnea. The average age was 45. Nearly half reported erectile dysfunction at baseline. After one, three, and six months of CPAP therapy, the majority showed measurable improvement in sexual function and satisfaction, including many who had not initially reported ED.
A more recent peer reviewed study published in Andrologia enrolled 133 men with suspected OSA. Of the 80 confirmed to have it, 60 percent reported erectile dysfunction. The authors identified strong correlations between erectile function and measures of apnea severity, oxygen saturation, and oxygen desaturation, and concluded that men with OSA are at significant risk of ED and should be screened for it.
Across the broader literature, the prevalence of ED among men with untreated obstructive sleep apnea is reported anywhere from roughly 40 percent to over 80 percent depending on the study population and the severity of apnea. That range is wide, but the floor is high. Whichever number you trust, ED is far more common among men with OSA than in the general population.
Why sleep apnea undermines sexual health There are at least four mechanisms running in parallel, and most patients have all of them at once.
The first is hormonal. Testosterone is produced on a sleep dependent rhythm in both men and women. It rises after sleep onset and reaches its highest levels during REM sleep. Sleep apnea fragments your nights and suppresses REM in particular, which can blunt the natural overnight testosterone surge. Lower testosterone can mean reduced libido for both sexes, and in men can also contribute to erectile difficulty. There is more on the link between mouth breathing, OSA, and testosterone on my page about mouth breathing, sleep apnea, and testosterone, since chronic mouth breathing seems to be its own contributor for some patients.
The second is vascular. Each apnea event drops your blood oxygen, sometimes severely. Over years of untreated OSA, those repeated drops contribute to endothelial dysfunction, which is the impaired ability of blood vessels to dilate properly. Erections rely on blood flow. So does arousal more broadly. When the vascular system has been quietly stressed every night for years, it shows up in the bedroom.
The third is autonomic. Untreated apnea keeps the sympathetic nervous system on high alert during sleep. That spillover into daytime physiology raises blood pressure, increases inflammation, and is generally not a good baseline for sexual response, which depends on the parasympathetic system being able to take over.
The fourth is the obvious one and probably the largest in practice: you are exhausted. Untreated sleep apnea produces the kind of fatigue that erodes interest in anything that requires energy or attention. The kind of sleep deprivation I lived with for years before diagnosis affects mood, patience, motivation, and intimacy in ways that are hard to fully appreciate from the inside. Add the irritability and low grade depression that often go along with chronic poor sleep and sex tends to fall off the priority list well before any specific dysfunction appears.
The piece men talk about: erectile dysfunction ED is the most studied corner of this topic, partly because it is the most measurable and partly because it is often the symptom that finally gets a man into a doctor’s office.
If you are dealing with both ED and snoring, daytime sleepiness, or an observed pause in breathing at night, sleep apnea deserves to be on the list before you settle on age, stress, or testosterone alone as the explanation. I go deeper into the specific physiological link on my page about sleep apnea and erectile dysfunction.
The encouraging part is that effective CPAP treatment improves erectile function for a meaningful share of men who use it consistently. The improvement is not instant. Most studies that show the effect look at three to six months of nightly use. That matches what I have heard anecdotally for years. People who push through the early adjustment period and become consistent CPAP users report a long list of quality of life improvements, and sexual function is on that list more often than CPAP marketing usually admits.
What it looks like for women Women’s experience with OSA is studied much less, but the data that exists points in a consistent direction.
Women with sleep apnea report lower scores on the Female Sexual Function Index, particularly in the desire, arousal, and satisfaction subscales. Underlying mechanisms overlap with men’s: disrupted sleep, hormonal imbalance, lower energy, and the mood effects of chronic poor sleep. What is different is the diagnostic side. Women with sleep apnea are systematically underdiagnosed because their symptoms tend to skew away from the loud snoring stereotype. They are more likely to report fatigue, insomnia, anxiety, or morning headaches than the textbook gasping arousal. Many are told they are stressed, perimenopausal, or simply tired, when the underlying issue is an airway that collapses during sleep.
If a woman is experiencing persistent fatigue and a quiet drop in interest or arousal, particularly alongside other classic OSA risk factors like weight gain, hypertension, or a history of snoring, sleep apnea is worth ruling out. An at home sleep apnea test is a low-friction way to start.
The early evidence on CPAP therapy in women suggests improvements in desire and arousal scores after sustained use, although the female-focused literature is still catching up. There is also a meaningful relationship benefit when the male partner with OSA gets treated. Quieter nights, better-rested partners, and reduced bedroom anxiety all matter, and they all tend to feed back into intimacy.
The relationship layer no one writes about, sex inside a long-term relationship, is rarely just about libido and blood flow. It is also about who you are sleeping next to, and what that experience has been like for both of you.
Untreated sleep apnea puts a partner through years of loud, jagged snoring punctuated by alarming silences. Many partners end up sleeping in another room. Resentment builds. Intimacy suffers from a slow erosion that has nothing to do with desire and everything to do with sleep deprivation on both sides of the bed. By the time the apnea is finally diagnosed, both people are running on a deficit.
Then there is CPAP itself, which carries its own baggage. The mask, the hose, the noise, the look of it. Some patients avoid starting therapy or quietly stop using it because they feel self-conscious in front of their partner. That is a real and human reaction, and it is worth surfacing rather than hiding. From everything I have heard over the years, most partners are relieved when the snoring stops. The mask quickly becomes invisible. What remains is a much better-rested person who is, frankly, more available in every sense of the word.
If the early days of CPAP feel awkward, that is normal. My post on overcoming CPAP anxiety covers what helped me get past the first stretch.
What actually helps The honest answer is that treating the sleep apnea is the lever that moves the most variables at once. Hormones, oxygenation, mood, energy, cardiovascular load. All of it shifts when you finally start sleeping properly.
CPAP therapy remains the most studied and most effective treatment for moderate to severe OSA. It is not the only option, but for most patients it is the first one a sleep physician will recommend. If you are new to it, my guide to using a CPAP machine walks through the basics. Consistency is what produces the change. Three nights a week is not enough. Most of the improvement studies were done on patients using CPAP nightly for at least three months.
Lifestyle changes complement the therapy rather than replacing it. Weight loss, when applicable, reduces apnea severity and improves vascular health on its own. Reducing alcohol, especially in the evening, reduces the depth of muscle relaxation that worsens apnea events overnight, and many CPAP users notice the change in their data on nights they have had a few drinks. Quitting smoking helps both airway inflammation and erectile function through cleaner vascular health. Regular cardiovascular exercise contributes on multiple fronts at once: better sleep architecture, healthier blood vessels, more stable mood, and improved hormonal balance. None of these are quick fixes, and none of them on their own are likely to be enough for moderate to severe sleep apnea, but they all stack with CPAP rather than competing with it.
If sexual symptoms persist after several months of consistent CPAP use, that is a conversation worth having with your doctor rather than something to push through silently. There are other contributors worth ruling out. Vascular disease, low testosterone independent of sleep, certain medications, hormonal shifts, depression, and relational factors can all play a role, and CPAP cannot fix those by itself.
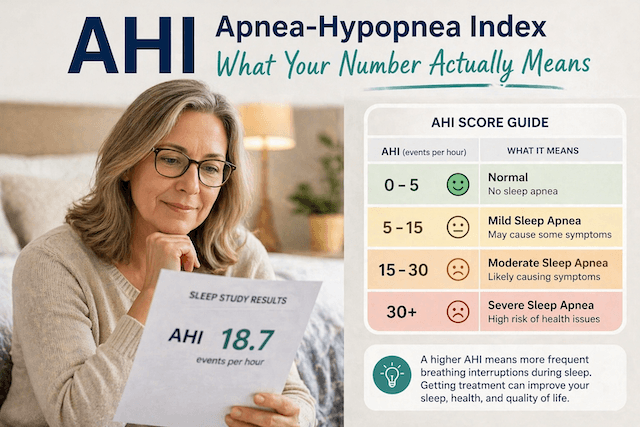
A note on getting tested If any of this resonates and you have not had a sleep study, that is the place to start. Diagnosis no longer requires a clinic stay in most cases. Modern home tests are accurate enough to identify OSA in the majority of patients, and they are far easier to commit to than an overnight in a sleep lab. I cover the full process on my page about sleep apnea diagnosis, along with the broader list of classic OSA symptoms worth checking against.
The reason I keep coming back to this is simple. Plenty of people I have talked to over the years started CPAP for a heart problem, a stroke risk, or a partner’s ultimatum about the snoring. Sexual health was rarely the trigger. But once they were sleeping properly, it was one of the things they noticed had quietly come back. It is not the most clinical reason to get tested. It is, for many people, one of the most personal.
The takeaway: Sleep apnea and sex are connected through hormones, blood flow, mood, and energy, and the connection runs in both directions. Untreated OSA can blunt libido, contribute to erectile dysfunction in men, and reduce desire and arousal in women. Effective treatment improves all of those, although not overnight, and only with consistent use.
If sex has quietly moved to the back of the queue, and you also snore, sleep poorly, wake up unrefreshed, or have any of the other classic symptoms of sleep apnea, it is worth investigating OSA as part of the picture. The conversation is awkward. The sleep study is not.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).