Hypopnea vs Sleep Apnea: Understanding the Key Differences
My Wake-Up Call: These are my sleep study results
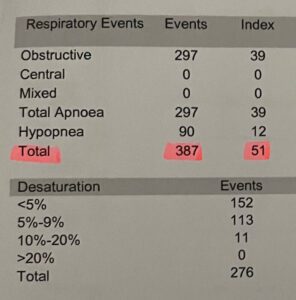
When I got my sleep study results back, most of the numbers made a kind of intuitive sense. Breathing events per hour. Oxygen saturation levels. Time spent in different sleep stages. But one word kept appearing alongside “apnea” in the report, and I had no idea what it meant: hypopnea.
My doctor explained it briefly, but I was taking in a lot of information that day and it didn’t fully land. It was only later, when I sat down and actually read through the report properly, that I understood what hypopneas were and why they were listed separately from the apneas. Once I understood the distinction, the whole picture of what had been happening while I slept made more sense.
If you’ve just received a sleep study report and you’re staring at the word hypopnea, wondering what it means and how it differs from sleep apnea, this is what I wish someone had explained to me clearly at the time.
What the Two Conditions Actually Are
Sleep apnea, specifically obstructive sleep apnea, is what most people have heard of. During an apnea event, your airway collapses completely. Airflow stops. Your oxygen levels drop, your body registers a threat, and you’re pulled partially awake to reopen the airway, usually with a gasp or snort. This can happen dozens or hundreds of times a night without you ever fully waking up or having any conscious memory of it.
Hypopnea is a partial version of the same problem. The airway doesn’t close completely but narrows enough that airflow is significantly restricted, typically by at least thirty percent of normal. Your breathing becomes shallow and ineffective. Oxygen still drops. You still get pulled out of restorative sleep. The mechanism and the consequences are similar to a full apnea, just less complete.
The simplest way I’ve found to think about it: an apnea is a blocked pipe, hypopnea is a kinked one. Neither is delivering what your body needs.
Both are counted together in the measurement you’ll see on your results, the Apnea-Hypopnea Index, which is the total number of apnea and hypopnea events per hour of sleep. That combined figure is what determines whether your sleep-disordered breathing is classified as mild, moderate or severe, and what treatment is recommended.
Why Hypopnea Matters as Much as Apnea
There’s a temptation, when you first understand the difference, to think of hypopneas as the less serious ones. Partial obstruction rather than full. Breathing reduced rather than stopped. That instinct is understandable, but the research doesn’t really support it. Studies comparing the health outcomes of patients with predominantly apnea events versus predominantly hypopnea events have found the consequences largely indistinguishable. Both cause oxygen desaturation. Both fragments sleep. Both carry the same cardiovascular and cognitive risks if left untreated.
What the research has also found is that for most patients, hypopneas are actually more frequent than full apneas. When I looked at my own results, that was true for me too: I had more hypopnea events than complete apneas, which meant a significant part of what was damaging my sleep and my health was this partial obstruction that I’d never even heard of.
This matters for treatment because CPAP addresses both. The pressurised air that keeps your airway open during sleep prevents the complete collapses that cause apneas and the partial collapses that cause hypopneas. Your CPAP therapy is treating both types of event simultaneously, which is part of why the AHI is expressed as a combined figure.
Reading Your Own Results
The AHI is broken down on most sleep study reports into its component parts. You’ll typically see an apnea index and a hypopnea index listed separately, then a combined AHI figure. The severity categories for adults are under five events per hour being normal, five to fourteen being mild, fifteen to twenty-nine being moderate, and thirty or above being severe.
If you’ve had an at-home sleep test rather than a full in-lab study, the numbers may be slightly underestimated because home tests calculate AHI based on total recording time rather than actual sleep time. If your home test came back mild but your symptoms are significant, it’s worth discussing a full polysomnography with your doctor.
The other number worth understanding on your report is the oxygen desaturation index, which measures how often your blood oxygen dropped below a certain threshold during the night. This adds context to the AHI because two people can have the same event count but very different oxygen profiles depending on how severe each individual event was.
What the Symptoms Look Like
The symptoms of hypopnea and sleep apnea overlap almost completely, which is one of the reasons people often don’t know which they have until they get a sleep study. Both cause fragmented sleep, morning headaches, excessive daytime fatigue, difficulty concentrating, and irritability. Both can contribute to depression and anxiety. Both put strain on the cardiovascular system over time.
The nighttime signs your partner might notice are slightly different. With a full apnea there’s typically a more obvious pattern: snoring, then silence as breathing stops, then a loud gasp or snort as it resumes. With hypopneas the snoring may be continuous but irregular and laboured rather than punctuated by silence. The pauses are less pronounced. But this distinction is subtle enough that even a partner who’s been watching you sleep won’t reliably know which is happening, which is why a sleep study is the only way to properly diagnose either.
I’d spent years assuming my snoring was just snoring. My wife had noticed the pattern I described above but neither of us knew what it meant. Looking back, the symptoms were unmistakable: morning headaches every day without fail, an inability to feel rested regardless of how long I slept, and a creeping fog through the afternoons that I’d been blaming on everything except the real cause.
Treatment: Both Conditions, Same Answer
For moderate to severe sleep-disordered breathing, whether the dominant events are apneas or hypopneas, the first-line treatment is CPAP. The machine delivers a continuous stream of pressurised air that acts as a pneumatic splint for your airway, preventing it from narrowing or collapsing regardless of the degree of obstruction. The pressure is calibrated to your specific needs, either set at a fixed level after a titration study or automatically adjusted throughout the night by an auto-titrating machine.
For mild sleep-disordered breathing, positional therapy is sometimes effective, particularly if your events cluster when you’re on your back. Weight loss reduces the soft tissue pressure on the airway and can significantly improve or in some cases resolve both apneas and hypopneas. Oral appliances that advance the lower jaw are a legitimate alternative to CPAP for people who can’t tolerate the machine, though they tend to be most effective for mild to moderate cases.
What doesn’t work is hoping the problem resolves on its own or deciding that because hypopneas are a partial obstruction rather than a complete one they’re not worth treating. The health consequences of untreated sleep-disordered breathing accumulate quietly over years. The stroke risk, the cardiovascular strain, the cognitive effects: these don’t care whether your AHI is composed primarily of apneas or hypopneas.
What Changed When I Started Treatment
I’ve written in more detail elsewhere about my first night with CPAP and the weeks that followed. The short version relevant here is that I felt the difference almost immediately. The morning headaches that had been part of my daily life for years began to fade within the first week. The afternoon fog lifted. I started waking up feeling like I’d actually slept rather than just survived the night.
What I understand now that I didn’t then is that both the apnea events and the hypopnea events on my sleep study were contributing to that damage. CPAP addressed both. The combined AHI that had been placing me in the severe category came down to a well-managed level, and the difference in how I functioned during the day reflected that improvement.
If you’re looking at a sleep study result with hypopneas listed and wondering whether they’re the part you need to worry about, the answer is yes. Not instead of the apneas, and not more than them, but alongside them. They’re part of the same condition and they respond to the same treatment.
What to Do If You Think You Have Either Condition
You can’t diagnose this yourself. Symptoms point toward the possibility, but the only way to know what’s happening during your sleep, and in what combination, is a proper sleep assessment. An at-home sleep test is a reasonable starting point for most people and your GP can refer you for one. If the results are inconclusive or your symptoms are complex, a full in-lab sleep study gives a more complete picture.
If you’ve already been diagnosed and you’re looking at the breakdown of apneas versus hypopneas on your report trying to understand what it means: both are being treated by your CPAP, both were contributing to your symptoms, and both will improve as your therapy stabilises. The ratio between them is less important than the combined AHI and how well your treatment is bringing that figure down.
The terminology can feel overwhelming when you first encounter it. Apnea, hypopnea, AHI, oxygen desaturation index: it’s a lot of new language arriving at the same time as a significant diagnosis. But the underlying picture, once you understand it, is actually fairly straightforward. Your airway was collapsing or narrowing during sleep more often than it should. That’s now being treated. Everything follows from that.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).