Blood Oxygen Levels During Sleep? What’s Normal?

Blood oxygen is one of those numbers that quietly governs how you feel, how you think, and how long your heart and brain stay healthy. Most people only encounter it as a brief reading at the doctor’s office, a quick clip on the finger and a value somewhere around 98 percent. It looks like a vital sign of passing interest. For anyone with untreated sleep apnea, it is one of the most important measurements in their life, even if they have never seen the number.
I am not a medical professional. My background is in computer science, and what I write comes from living with severe obstructive sleep apnea for more than a decade, paying close attention to my own therapy data, and reading the relevant clinical literature with the curiosity of someone whose life depends on understanding it. My diagnosis came after years of warning signs that I did not connect at the time. The full story sits on a separate page, Living with Sleep Apnea. The short version is that my AHI was 51 when I was finally tested, which is severe by any classification system. Severe AHI carries severe overnight oxygen consequences, and that is what this page is about.
What Blood Oxygen Actually Is
Blood oxygen saturation, almost always written as SpO2, measures the percentage of hemoglobin in your blood that is actively carrying oxygen. Hemoglobin is the protein in red blood cells that binds to oxygen molecules in the lungs and releases them where the body needs them. When SpO2 is 98 percent, almost every red cell passing through the lungs is fully loaded. When it falls to 88, a substantial fraction is no longer carrying its share. The brain, the heart, the kidneys, every working tissue depends on a steady supply, and the body has very little tolerance for repeated drops.
Cleveland Clinic puts the threshold for clinical concern around 90 percent and describes hypoxemia as a state where oxygen levels in the blood are lower than normal, which over time can lead to organ damage. That framing is worth holding onto when looking at sleep apnea, because a single dip below 90 is not the issue. The issue is the pattern.
What a Normal Night Looks Like
For a healthy adult, blood oxygen during sleep generally sits in the same range as during the day. Most reliable medical sources put the normal range at 95 to 100 percent SpO2 throughout the night, with brief, shallow dips into the low 90s during REM sleep considered acceptable. REM is the stage where the muscles, including those involved in breathing, are most relaxed. Breathing becomes a little less regular, oxygen wavers a little, and then the body recovers without any conscious involvement on your part.
What is not normal is repeated, significant desaturation. Drops into the 80s, or lower, happening dozens or hundreds of times across a single night, are not part of a healthy sleep cycle. They are a sign that something is interfering with airflow.
Why Sleep Apnea Pulls Oxygen Down
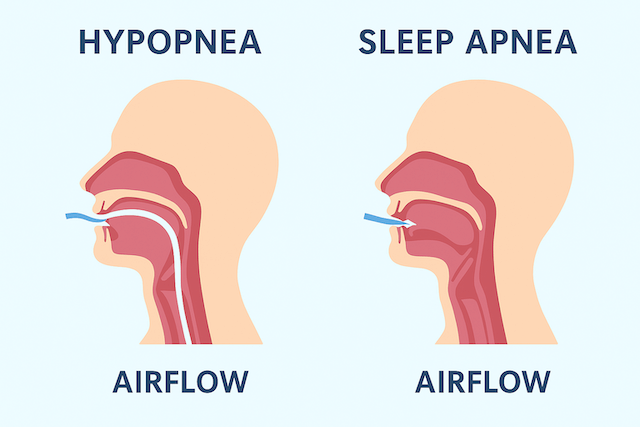
The mechanism in obstructive sleep apnea is mechanical and straightforward. When you fall asleep, the muscles of the upper airway relax. In people with OSA, that relaxation goes far enough that the soft tissue at the back of the throat collapses inward. The airway narrows, or closes entirely. Airflow drops or stops. No air reaches the lungs, no oxygen enters the bloodstream, and the SpO2 reading begins to fall.
The brain notices. It triggers a brief arousal, just enough to restore muscle tone, reopen the airway, and restart breathing. You gasp, often without remembering it, and slip back into sleep. Then the cycle starts again. With an apnea hypopnea index in the severe range, this is happening roughly once a minute, all night, for as long as the condition is untreated. That is the engine behind the oxygen pattern that shows up on a sleep study report.
Central sleep apnea produces a similar oxygen picture through a different mechanism. The airway is open, but the brain fails to send the breathing muscles a signal to inhale. The pause in breathing is the same. The oxygen drops the same way. The treatments differ, which is one of the reasons it is important to get a proper diagnosis rather than guessing from symptoms.
Other things can drive low overnight oxygen as well. Chronic lung disease, particularly COPD, reduces the lungs’ ability to transfer oxygen into the bloodstream, and the combination of COPD and sleep apnea is sometimes called overlap syndrome, with an especially poor oxygen profile. Severe obesity can cause sleep related hypoventilation, where breathing is simply too shallow to maintain healthy oxygen levels. At very high altitude, baseline oxygen is naturally lower for everyone. Sleep apnea is one cause among several, but it is by far the most common explanation for repeated overnight desaturation in otherwise healthy adults.
What Repeated Desaturation Does to Your Body
A single oxygen dip is not dangerous on its own. The body recovers without consequence, the way it recovers from any number of small physiological disturbances throughout a day. The problem with sleep apnea is repetition. Hundreds of small emergencies, every night, for years, do compound.
The cardiovascular system bears a particular share of that load. Each desaturation prompts the body to constrict blood vessels and raise blood pressure to redistribute the oxygen that is left. The heart works harder, repeatedly, through an emergency response, and the chronic stress on the cardiovascular system is one of the main reasons untreated sleep apnea is associated with elevated risk of high blood pressure, heart arrhythmias, and other cardiovascular events. The American Sleep Apnea Association lays out the connection in plain terms in their overview of oxygen during sleep, and the clinical research behind it is substantial.
The brain is the other major casualty. It uses roughly a fifth of the body’s total oxygen supply and is particularly vulnerable to the kind of repeated deprivation that untreated sleep apnea creates. The fog that so many untreated patients describe, the difficulty concentrating, the memory that no longer holds detail, the conversations that simply do not stick, is partly what oxygen deprivation across thousands of nights does to cognitive function. This is one of the reasons sleep apnea is associated with elevated stroke risk. Years of blood pressure spikes and oxygen drops damage the blood vessels that supply the brain.
For me personally, one of the most striking signals in retrospect was a pattern of severe morning migraines. They resolved with treatment, and the resolution is one of the things I find most telling when I look back at the years before diagnosis. Oxygen deprivation has fingerprints all over how you feel during the day, and many of them are not obviously about breathing.
How Oxygen Gets Measured When You Sleep
Pulse oximetry is the most common way to monitor SpO2. A small device clips to the finger and uses two wavelengths of light to estimate the proportion of hemoglobin carrying oxygen. It is noninvasive, painless, and continuous, which is why it is built into nearly every sleep study and overnight monitoring device on the market.
Standalone overnight pulse oximetry can be a useful screening tool, but it is not a diagnostic test on its own. It can tell you whether your oxygen is dropping, but not why. If the answer is yes, you generally need a full sleep evaluation to determine the cause. A consumer pulse oximeter from a reputable medical brand can give you a rough overnight picture, but the cheap, unvalidated devices sold online are often inaccurate in ways that are difficult to spot from the outside. If you are spending money on one, spend it on a device that meets accepted medical standards.
An in lab sleep study captures far more than oxygen. It records brain wave activity, heart rhythm, breathing effort, body position, leg movement, and airflow, all simultaneously, alongside SpO2. That combination is what allows a sleep specialist to identify exactly what kind of breathing event is occurring, when in the sleep cycle it happens, and what is driving the oxygen pattern. An at home sleep test covers less ground but is convenient, accessible, and capable of confirming or strongly suggesting sleep apnea in someone with reasonable symptoms. For many people, an at home test is the right first step.
Once you are in treatment, modern CPAP machines track therapy data continuously, including residual events and, in some configurations, oxygen saturation. I check my data through the ResMed app every morning, and the habit is now as automatic as glancing at the weather forecast. The reading is part of how I know my therapy is working and how I would catch a problem early if something started to slip. Tools like OSCAR can pull out more detailed views for anyone who wants to read their own data more closely.
What CPAP Therapy Does to the Oxygen Picture
For moderate to severe obstructive sleep apnea with significant desaturation, CPAP is the standard treatment for a reason. The mechanism is simple. A stream of pressurized air, delivered through a mask, holds the airway open during sleep so the soft tissue cannot collapse inward. With the airway open, airflow continues uninterrupted, oxygen exchange in the lungs continues uninterrupted, and the cascade of arousals and desaturations does not happen.
What the contrast looks like, for someone moving from severe untreated disease into properly titrated therapy, is dramatic. The events stop, or near enough to stop that the difference is unmistakable in the data. Oxygen sits in the healthy range through the night rather than swinging in and out of it. The morning headaches I lived with for years simply went away once my therapy was established, and they have not come back. The fog that I had taken for a permanent feature of how my brain worked turned out not to be permanent. The exhaustion I had assumed was a baseline turned out not to be a baseline.
I use a ResMed AirSense 10 with a full face mask, since I am a chronic mouth breather and a nasal mask was never going to work for me. The early weeks of CPAP took adjustment, in the way that starting any new therapy takes adjustment. Most of what I worked through is documented in my troubleshooting guide. The initial discomfort settled. The underlying improvement did not, and it has held over a decade of consistent use.
Other Factors That Affect Overnight Oxygen
CPAP does the heaviest lifting for severe sleep apnea, but a number of other factors influence how your oxygen behaves at night, and several of them are worth knowing about even if you are already in therapy.
Sleep position is the most underrated of these. Sleeping on your back allows the tongue and soft palate to fall backward and narrow the airway more easily, which means more events and deeper desaturations. Side sleeping keeps the airway more open and, for many people, reduces both event frequency and the depth of any drops that do occur. My page on the best sleeping position for sleep apnea covers the practical side of this in more detail.
Alcohol within several hours of bedtime relaxes the throat muscles beyond their normal sleep state. For someone with sleep apnea, that means more frequent and more severe events than the same person would have on a dry night. Some people do not realize how much an evening drink is moving their numbers until they look at the data side by side.
Nasal congestion, whether from allergies, a cold, or a structural issue like a deviated septum, pushes you toward mouth breathing and disrupts the way air moves into the lungs. Treating chronic congestion will not solve obstructive sleep apnea on its own, but it often softens the overall airway picture and makes CPAP more comfortable, particularly for nasal mask users.
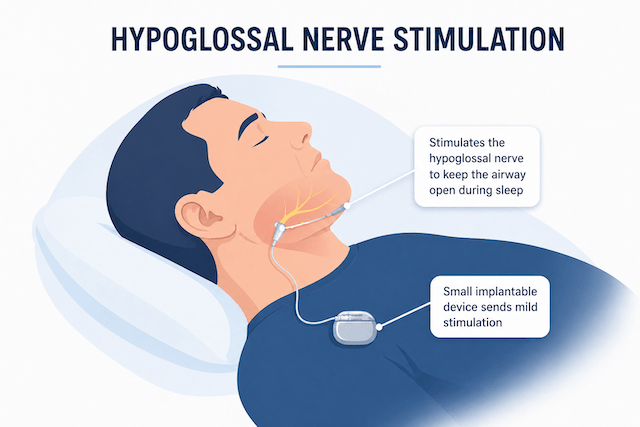
If CPAP is genuinely not an option for someone, alternative treatments do exist. Oral appliances that reposition the jaw work for some milder cases. Hypoglossal nerve stimulation is a surgical option for carefully selected patients who cannot tolerate PAP therapy at all. For severe disease with significant overnight desaturation, the evidence behind these alternatives is thinner than the evidence behind CPAP, and that gap is worth understanding before walking away from CPAP because the first few nights felt strange. My page on CPAP anxiety covers a lot of what gets people through the early adjustment period.
How to Tell If Your Own Oxygen Might Be Dropping
The honest answer is that you usually cannot tell from symptoms alone. The desaturations happen while you are asleep. You have no direct experience of them. What you feel is the downstream consequence: the exhaustion that no amount of caffeine fixes, the morning headaches, the fog that does not lift, the moodiness, the slower reaction times, the partner who has started sleeping in another room because the snoring is unbearable.
If someone who sleeps near you has described watching you stop breathing, that is the clearest signal there is, and it is worth acting on promptly. Daytime sleepiness that does not respond to longer sleep, regular morning headaches, blood pressure that has been creeping up without an obvious explanation, or a general sense that your thinking is not what it used to be are all worth raising with your doctor and asking specifically about sleep apnea. A home sleep test is a reasonable starting point, and tends to be far less daunting than people expect.
The number on the oximeter is not the whole story, but it is a useful entry point. You cannot treat what you have not measured, and getting an actual reading is the move that opens up everything else. The years of feeling broken before my diagnosis and the years of feeling normal again afterward sit on either side of that one decision to find out what was actually happening to me at night.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).