Sleep Respiratory Rate: What It Is and What CPAP Changed for Me

I was diagnosed with severe obstructive sleep apnea more than a decade ago, with an AHI of 51 at diagnosis. My wife was the one who first noticed that my breathing at night was not normal, and that was the push that finally got me into a sleep study. I will not retell that whole story here, because I covered it in living with sleep apnea. What I want to do on this page is explain something that confused me for a long time: sleep respiratory rate. What it is, why it matters for a sleep apnea diagnosis, and what actually changed for me after more than a decade of CPAP therapy.
One thing up front. My background is in computer science, not medicine. I am a patient who has lived with this condition for a long time, not a clinician. Everything medical here is drawn from research and from what my doctors have explained to me, and I will keep what I have personally experienced clearly separate from what is simply reported. If you are worried about your own breathing during sleep, the right move is a conversation with a doctor and a proper sleep study, not a blog post.
What Sleep Respiratory Rate Actually Means
Your sleep respiratory rate is simply the number of breaths you take per minute while you are asleep. It sounds basic, and it is, but it turns out to be one of the vital signs clinicians pay attention to, alongside heart rate, blood pressure, and oxygen levels. When you have a condition like sleep apnea, the pattern of your breathing during sleep stops looking the way healthy breathing should.
Before I understood any of the terminology, I just knew I felt terrible. I woke up unrested no matter how long I had been in bed, and I had headaches almost every morning. I did not have a word for it, but my breathing during sleep was clearly not doing what it was supposed to. The point worth making is that you do not feel your respiratory rate directly. You feel the downstream effects of breathing that keeps getting interrupted, which is what sent me looking for answers in the first place. If you want the broader picture of the condition itself, I wrote a plain language explainer on what sleep apnea is.
What Is a Normal Respiratory Rate While Sleeping?
For most healthy adults, a normal respiratory rate at rest sits somewhere around 12 to 20 breaths per minute, according to general clinical references like the Cleveland Clinic. The exact figure shifts with age, and children and older adults can run a bit differently. Here is a rough reference range that is commonly cited:
| Age range | Typical breaths per minute |
|---|---|
| Children (6 to 12 years) | 16 to 24 |
| Teens (12 to 17 years) | 13 to 21 |
| Adults (18 to 65 years) | 12 to 20 |
| Older adults (65+ years) | 12 to 28 |
The number matters less than the word that should sit next to it: steady. Healthy breathing during sleep is regular, with gentle shifts across different sleep stages. It tends to slow a little in deep sleep and pick up slightly during REM. Those are smooth transitions, not the dramatic spikes and crashes you see with untreated sleep apnea. The Sleep Foundation has a good overview of why consistency, rather than a single magic number, is the thing that tells you breathing is healthy.
How Sleep Apnea Disrupts the Pattern
This is where respiratory rate stops being a tidy number on a chart. With obstructive sleep apnea, the airway narrows or collapses during sleep. Breathing slows or stops entirely for a stretch, then the body reacts to the falling oxygen and rising carbon dioxide by jolting you toward wakefulness so you can catch up. The result is a sawtooth pattern rather than a steady line: pauses, then a rush of faster, harder breathing as the body tries to repay the oxygen debt, then back around again.
Clinicians sometimes describe that catch up breathing as compensatory hyperventilation. The practical takeaway is that an apnea is not just a quiet gap. It is a stop followed by a struggle, repeated over and over through the night. That cycling is the reason people with untreated apnea can spend eight or nine hours in bed and still wake up feeling like they never rested. The body never settles into the slow, even breathing that real recovery depends on.
My own diagnosis put a number on how often this was happening to me. An AHI of 51 means roughly 51 breathing events per hour, which lands in the severe range. I did not need to know my exact breaths per minute to understand the picture. The events themselves told the story.
The Signs That Sent Me Looking for Answers
You do not need a sleep study to suspect that something is wrong with your breathing at night, although you do need one to confirm it. These are the warning signs that commonly point to disordered breathing during sleep. Some of them I lived with directly. Others are simply the established list, and I want to be clear about which is which.
The two that hit me hardest were morning headaches and constant fatigue. I woke up with a headache almost every day and assumed it was stress or just getting older. It was neither. When breathing is repeatedly interrupted, carbon dioxide builds up overnight, and morning headaches are a classic result. The fatigue was the other one. I could sleep a full night and still feel wrung out, because my body was working hard all night instead of resting. I also had high blood pressure around the time I was diagnosed, which is a well-documented companion to untreated sleep apnea.
Beyond what I experienced, the broader symptom list is worth knowing. People with disordered breathing often report waking up gasping or choking, a dry mouth or sore throat in the morning, frequent trips to the bathroom overnight, and a racing heart. During the day it can show up as brain fog, irritability, and falling asleep when you should not, such as in meetings or behind the wheel. A bed partner is often the first to notice the loudest signs: heavy snoring that stops and starts, audible pauses, and restless, thrashing sleep. My wife noticing my breathing is exactly how this got taken seriously in my house.
If several of these sound familiar, I put together a more detailed walk through of sleep apnea symptoms, and a gut check piece on whether you might have sleep apnea. Neither replaces testing, but both can help you decide whether to push for it.
How a Sleep Study Measures Your Breathing
When I went through testing, I learned that a sleep study does not just count breaths. It builds a full picture of what your respiratory system is doing. Bands around the chest and abdomen measure breathing effort, a sensor at the nose measures actual airflow, and a pulse oximeter tracks blood oxygen. Put together, those signals show how often breathing pauses or goes shallow, how far oxygen drops, and how all of that lines up with your sleep stages.
That combination is what produced my diagnosis. The individual measurements matter less than the pattern they reveal, which in my case was a high number of events per hour and the disrupted breathing that comes with severe obstructive sleep apnea. You can start with an at home sleep test or go straight to a full sleep lab study, and your doctor can help you decide which fits your situation. If you want to understand the headline number that comes out of it, my page on the AHI, the apnea hypopnea index, breaks it down.
How CPAP Changed Things for Me
Here is a point that surprised me, and it is worth stating plainly because the original version of this article got it wrong. Standard CPAP machines do not display your respiratory rate on screen. They report the metrics you can actually act on, like AHI and mask leak. So I cannot tell you that I watched my breaths per minute tick down on a display, because no such display exists on the machines most of us use. What I can tell you is what changed in how I felt and what my CPAP data shows.
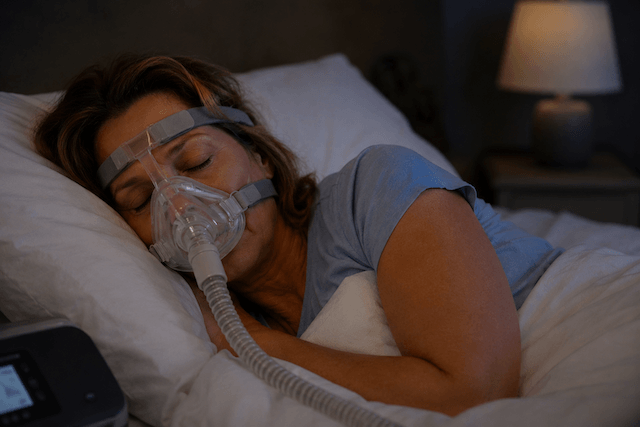
CPAP works by delivering a steady stream of air pressure that holds the airway open, which prevents the collapses that cause apneas in the first place. My first night with CPAP was strange. The mask felt unfamiliar and I was aware of every breath. But the gasping and the broken sleep eased far faster than I expected. Within the first couple of weeks the morning headaches were gone, and they have stayed gone unless I am actually sick.
The adjustment period is real, and it is not always smooth. Getting used to CPAP therapy took some patience, and plenty of people hit a wall of frustration early on. If that is you, I wrote about overcoming the anxiety that tends to show up in the first months. Pushing through it was worth it. My treated AHI now sits consistently under five, which is the range you are aiming for, and the day-to-day difference is the part that actually matters to me. I wake up rested. I have energy that does not vanish by mid-morning. My wife is not lying awake listening to me stop breathing.
After more than a decade, I do not track my respiratory rate at all. I pay attention to how I feel when I wake up; I glance at my AHI and leak rate in the app, and I see my sleep doctor for a check now and then. That has been enough. As a chronic mouth breather, I use a full face mask, which is the only setup that ever made sense for me, and I run a ResMed AirSense 10 at home with a travel machine for trips and camping. I am currently weighing an upgrade to the AirSense 11, though I have not pulled the trigger yet.
Respiratory Rate and the Different Types of Sleep Apnea
Understanding respiratory rate also helped me understand the different forms the condition can take, because the breathing pattern looks different depending on the cause.
With obstructive sleep apnea, which is what I have, the airway physically collapses. The telltale sign is that the body keeps trying to breathe. The chest and abdomen are still working, but no air is moving, so effort ramps up until an arousal finally reopens the airway with a sudden gasp.
With central sleep apnea, the problem is different. The brain briefly stops sending the signal to breathe, so there is no effort at all during the pause. Some people develop central events while on CPAP, a situation sometimes called complex or mixed sleep apnea, and when that happens the treatment can change, occasionally moving toward ASV therapy rather than standard CPAP.
Then there are hypopneas, which are partial reductions rather than full stops. Breathing keeps going but turns shallow, and the body has to work harder to pull in enough oxygen. My own pattern included plenty of these, not just complete pauses. That is why the AHI counts both apneas and hypopneas: shallow, inadequate breathing matters too.
What Makes Breathing During Sleep Better or Worse
Over the years I have noticed, and the research backs up, that several everyday factors influence how easily you breathe at night.
Sleeping position is a big one. Lying on your back lets the tongue and soft tissues fall back and crowd the airway, which makes obstruction worse. Side sleeping generally helps, and the best sleeping position for sleep apnea is something I had to train myself into. Body weight plays a role as well, and there is a documented link between weight and the airway, which is why weight changes can shift how therapy feels over time. Alcohol before bed relaxes the throat muscles and tends to make obstruction worse, so it is worth being mindful of in the evening. Nasal congestion from a cold or allergies makes you work harder to move air, which is part of why I wrote a guide on using CPAP when sick. And a hot, stuffy room never helps, both for comfort and because it can contribute to CPAP rainout in the tubing.
None of these replace treatment. They are the kind of small adjustments that make good therapy work a little better.
Do You Need to Track Your Respiratory Rate at Home?
My honest answer, after living with this for a long time, is probably not. Unless a doctor has a specific reason to ask you to, obsessively tracking breaths per minute at home is not where I would put my attention. What I watch instead is how I feel in the morning, whether old symptoms are creeping back, my CPAP compliance and data, and my AHI and events per hour.
If you do want some passive insight, a few consumer devices estimate respiratory rate during sleep, including the Apple Watch with its sleep apnea detection feature and various fitness trackers, with accuracy that varies. For an actual screening rather than a wellness estimate, a home test like the WatchPAT One is a different category of tool. But none of these diagnose sleep apnea. Diagnosis comes from a proper sleep study, and ongoing reassurance comes from how you feel plus the data your machine already gives you.
When to Talk to a Doctor
If you have never been tested and you recognize the symptoms, gasping at night, loud stop-and-start snoring, relentless daytime fatigue, morning headaches, do not sit on it. Early diagnosis and treatment make a real difference, and there are several paths forward worth understanding, which I cover in my overview of alternative treatments for sleep apnea.
If you are already diagnosed and using CPAP, reasons to check in with your doctor include old symptoms returning, a sense that the machine is no longer doing its job, a meaningful change in your AHI, real trouble staying consistent, or a significant change in weight. And anything that feels like a genuine breathing emergency, such as new chest pain or severe shortness of breath, is a reason to seek care right away rather than wait.
The Bottom Line
After more than a decade with diagnosed sleep apnea, here is what I have actually learned about respiratory rate during sleep. The exact number of breaths per minute matters far less than whether your breathing is steady, and you cannot judge that from a CPAP screen because standard machines do not report it. Sleep studies are where the real breathing data and the real diagnosis come from. Consistent CPAP use genuinely normalizes disrupted breathing, and for me the proof is not a chart but the simple fact that I wake up rested and stopped thinking about my breathing at all. And the symptoms- the gasping, the headaches, the bone-deep fatigue- matter more than any number, because they are your body telling you something is wrong.
If that sounds like you, please get tested. If you have been tested and you are struggling with treatment, stick with it. From someone who spent years feeling exhausted and now does not, it is worth it.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).