The Future of ASV Technology: How this Technology Might Evolve
I want to say up front what this post is and is not. I have lived with severe obstructive sleep apnea for more than a decade. I am a daily CPAP user, not an ASV user. My background is computer science, not medicine. So this is not a clinician’s view of where adaptive servo ventilation is heading, and it is not a personal review of a machine I have used at home. It is a long time CPAP patient with a software brain looking at the public research on ASV and trying to honestly read where the technology is going, what is real, and what is still mostly hope.
Adaptive servo ventilation, usually shortened to ASV, is the closest thing in mainstream sleep medicine to a machine that thinks while you breathe. Where my ResMed AirSense 10 sits in CPAP territory and holds a steady pressure, an ASV machine watches each breath and adjusts pressure support in real time. It is mainly used for central sleep apnea, Cheyne-Stokes respiration, complex sleep apnea, and treatment emergent central apnea, conditions where standard CPAP often falls short or makes the breathing pattern worse. If you want the foundation, my page on what ASV is covers the basics, and the ASV vs BiPAP vs CPAP page sets out the differences.
This post looks ahead at where ASV is most likely to go in the next several years and where the public evidence supports those predictions.
Where ASV stands right now
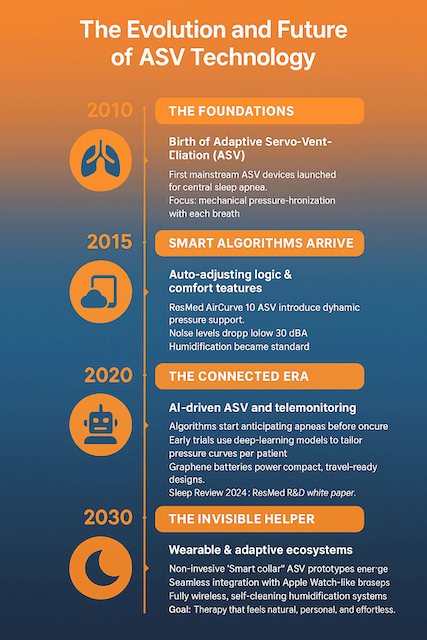
The current generation of ASV machines, including the ResMed AirCurve 11 ASV and the Philips DreamStation BiPAP autoSV, is already doing things that would have sounded like science fiction when I started CPAP therapy. They sample airflow many times per second, recognize the difference between an obstructive event, a central event, and Cheyne-Stokes breathing, and modulate inspiratory pressure to stabilize the patient’s pattern. They report data to the cloud for clinicians to review. They run quietly enough to share a bedroom. The mechanical and algorithmic core of what an ASV machine does has matured a lot in the last ten years, and you can read more about how ASV works in my deeper write up.
That is the good news. The harder news is that ASV has had a serious safety story attached to it for the better part of a decade, and any honest forward look has to start there. In 2015, the SERVE-HF trial published in the New England Journal of Medicine studied 1,325 patients with chronic heart failure, a left ventricular ejection fraction of 45 percent or less, and predominantly central sleep apnea. After a median follow-up of 31 months, the ASV group showed a roughly 34 percent increase in the risk of cardiovascular death compared with the control group, even though ASV controlled their central events well. In response, the American Academy of Sleep Medicine published a Standard level recommendation against using ASV to treat central sleep apnea associated with congestive heart failure in patients with that ejection fraction profile. The AASM updated its broader guidance for central sleep apnea again in 2025.
So when I think about the future of ASV, I do not start with the futurist material. I start with the fact that the technology is genuinely useful for a defined patient population, and genuinely contraindicated for another, and that the most important short term progress is probably better patient selection, not flashier features. None of this is medical advice. It is the public, peer reviewed picture as I read it. If you are working through whether ASV is even the right category for your situation, the ASV machines overview and the ASV therapy for other health conditions page are reasonable starting points.
The real AI story is more boring, and more useful, than the hype
You will see plenty of marketing about artificial intelligence in sleep therapy. Most of it is overselling. A small piece of it is real, and the real piece is genuinely interesting.
The clearest example is ResMed’s Smart Comfort, which received FDA 510(k) clearance in December 2025. Smart Comfort is a machine learning system trained on more than 100 million nights of de-identified sleep data. It does not change your prescribed pressure. What it does is recommend personalized comfort settings on top of that prescription, things like ramp behavior and the way the device handles pressure on exhale, based on patterns that show up across very large populations. A limited beta on the AirSense 11 launched in early 2026 for new myAir users. That is, at the time I am writing this, the first FDA cleared AI enabled medical device of its kind in CPAP territory.
Smart Comfort is a CPAP feature, not an ASV feature, but the direction of travel is what matters. It tells you something honest about where this is going. The near term win is not a machine that predicts your apneas before they happen. It is a machine that uses population scale data to nudge comfort and adherence settings, where the evidence is strongest. The bigger leaps, predictive event modeling and personalized algorithm tuning specifically for ASV, are plausible but not yet here. When researchers do publish that work, I will believe it. Until then, I treat anything dressed up in the language of “AI ASV” as marketing.
For people who already use connected machines, the practical version of this future shows up in tools like myAir and AirView, where therapy data flows to the cloud and clinicians can adjust settings remotely. If you want to understand your own data, my walkthrough on how to interpret CPAP data and the page on ASV therapy data tracking cover where to start. The OSCAR community software is also worth knowing about for users who want a deeper read of their own nightly patterns.
Remote care will get better, but the evidence is mixed
Telehealth in sleep medicine is one of those areas where the marketing has run ahead of the data, but the data is real and improving.
A 2021 meta analysis of eleven randomized controlled trials, totaling more than 1,300 patients, found that telemedicine interventions during the first six months of CPAP therapy improved adherence by an average of about half an hour per night. The Tele-OSA trial, published in the American Journal of Respiratory and Critical Care Medicine in 2018, randomized 1,455 patients across four arms and found that CPAP telemonitoring with automated feedback messaging improved 90 day adherence. Other trials have found no significant difference between telemonitoring and standard care once both groups are well managed.
What that mixed picture tells me is that connectivity by itself is not the win. Connectivity plus a thoughtful protocol that actually responds to the data is the win. For ASV patients, where the prescribed therapy is more complex than CPAP and the consequences of poor titration are larger, that pattern probably matters more, not less. The plausible future is shorter feedback loops between patient and clinician, fewer in person titration visits for patients who do not need them, and earlier intervention when therapy quality is slipping.
For people in remote areas, including parts of regional Australia where I live, that change cannot come fast enough. A clinician should not need you to drive five hours to adjust a setting that the cloud could surface in five minutes.
Smaller, lighter, and more travel friendly
ASV machines today are bulky compared with travel CPAPs. My ResMed AirMini is small enough to throw in a backpack. Nothing on the ASV side comes close yet.
That gap will narrow. Brushless motor design has been improving steadily across the industry. Battery chemistry, particularly lithium iron phosphate, keeps getting more energy dense and safer. The mechanical work that an ASV machine has to do is not fundamentally different from what a travel CPAP does. It is the algorithm and sensor fidelity that distinguish it. Once the comfort features that sit around the core motor, particularly humidification, become more compact, an ASV in the size class of a current travel CPAP becomes engineering, not invention.
I am cautious about putting a date on it. ASV is a smaller market than CPAP, which means less commercial pressure to miniaturize. But I would be surprised if we did not see meaningfully smaller travel-oriented ASV options before the end of the decade. The first time someone with central sleep apnea can take a real ASV class machine on a camping trip without hauling a small suitcase, that will be a quiet but important shift.
Comfort and humidification are still the limiting factors
The most advanced therapy in the world fails if people will not wear it. The biggest reasons people abandon PAP therapy are not algorithmic. They are dry mouth, mask leak, claustrophobia, and the steady annoyance of running a hose to your face every night. Anyone who has spent time on this site knows I have written about CPAP anxiety from personal experience, and that early friction nearly cost me therapy entirely.
The plausible near term improvements here are not glamorous, but they would matter. Heated tubing systems that respond to ambient bedroom conditions automatically rather than relying on a fixed climate setting. Better closed loop humidification that adjusts moisture in response to nasal flow rather than a single user picked level. Mask materials that hold their seal under more head movement, reducing the leak alarms that wake patients up in the small hours.
ResMed’s existing Climate Control feature already does some of this on current AirSense and AirCurve devices. The future direction is more sensors, more closed loop control, and probably the same comfort improvements showing up first on CPAP and only later on ASV. That is the usual pattern. Volume drives iteration, and CPAP is where the volume is.
Beyond the mask: where ASV territory might split
The most interesting longer term question is whether the future of central sleep apnea care is still mask based at all.
The remedē System, made by ZOLL, is an FDA approved implantable device that delivers transvenous phrenic nerve stimulation to treat moderate to severe central sleep apnea in adults. The original device was approved in 2017, and a next generation EL-X version was approved more recently. The 2025 AASM clinical practice guideline on central sleep apnea includes transvenous phrenic nerve stimulation as a recommended treatment option. It is implanted in the chest, activates automatically each night, stimulates the phrenic nerve, and triggers the diaphragm to maintain a more normal breathing pattern. There is no mask. There is no hose. There is no humidifier.
That is a meaningful divergence from the ASV path. ASV will likely remain the right choice for many patients, particularly those with predominantly obstructive components, treatment emergent central apnea, or patients who do not want surgery. But for some of the population that current ASV serves, especially those for whom the SERVE-HF data complicates the picture, an implanted alternative is going to be part of the conversation.
The same broad theme shows up on the obstructive side, where the Inspire hypoglossal nerve stimulation implant has been treating obstructive sleep apnea for years. I have a deeper write up on hypoglossal nerve stimulation and on EPAP therapy if you want to look at the broader landscape of alternative treatments for sleep apnea.
The point is that the future of ASV probably is not just better ASV. It is a wider menu of options, including some that do not look like ASV at all, with better tools to match the right patient to the right therapy. Sometimes the right therapy will still be a refined ASV machine. Sometimes it will be something else entirely.
Real challenges, not invented ones
Anyone writing about future medical technology has a responsibility to flag the harder parts honestly.
Cost and access is the first one. AI augmented and connected devices have a tendency to be priced higher, at least at launch. ASV machines are already significantly more expensive than CPAPs, and insurance coverage rules vary widely. Connectivity features that require a data plan or app subscription introduce another layer. If the next generation of ASV gets smarter but also gets harder to afford, the patient population that benefits the most may end up with the worst access.
Data privacy is the second. Connected sleep devices generate a remarkably detailed picture of a person’s life. Sleep timing, breathing irregularities, weight changes inferred over time, even rough indicators of alcohol or illness on a given night. The legal and ethical frameworks for that data are still catching up. Anyone using a cloud connected machine should know who can see what data, for what purpose, and for how long.
Regulation and validation is the third. The FDA path for AI enabled medical devices is still being worked out, particularly for systems that learn or update after deployment. Smart Comfort was cleared as a fixed function tool, not a continuously learning system. The harder question, how to safely validate a device that adapts on its own, is not yet solved. That is not a reason to be cynical, but it is a reason to be patient about the timeline.
The fourth is the SERVE-HF lesson itself. The single most important insight of the last decade in ASV is that a therapy that controls the surface physiology can still harm a specific patient population. Good clinical decisions depend on good selection, not just on good machines. No amount of machine learning will fix a mismatch between the therapy and the patient.
What I think actually changes
Stripping out the hype, here is what I think is reasonably likely over the next handful of years.
ASV machines themselves will get quieter, more compact, and better at telling clinicians and patients what is happening over time. Their core algorithms will improve incrementally rather than dramatically. The biggest changes for everyday users will come from the surrounding ecosystem: better remote monitoring, better comfort tuning, better data tools, better integration with consumer wearables like the Apple Watch sleep apnea detection feature. There will likely be at least one credible travel sized ASV option before the end of the decade, even if it does not match the AirMini for size.
Outside the ASV box, transvenous phrenic nerve stimulation will keep growing as a real alternative for the right patients with central sleep apnea, particularly those flagged by SERVE-HF as poor candidates for ASV. Hypoglossal nerve stimulation will keep growing on the obstructive side. The category that today is “ASV” will gradually become a smaller slice of a more diverse therapy landscape.
For people like me, who have been using a mask every night for years, the most important shift is the boring one. Therapy that is easier to start, easier to stick with, and easier to share with a clinician across distance. That is where the public evidence is strongest, and that is what would have made the worst parts of my own first year on therapy easier to get through. If you are at the start of your own journey, my page on living with sleep apnea is the better place to begin than this one.
The future of ASV is not a fantasy of a machine that knows you. It is a steady set of improvements that, taken together, make a difficult therapy a little less difficult. From where I sit, after more than a decade on CPAP, that is enough.
Sources and further reading: Cowie MR et al., “Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure,” New England Journal of Medicine, 2015. Aurora RN et al., “Updated Adaptive Servo-Ventilation Recommendations for the 2012 AASM Guideline,” Journal of Clinical Sleep Medicine, 2016. Badr MS et al., AASM 2025 clinical practice guideline on the treatment of central sleep apnea in adults. Hwang D et al., “Effect of Telemedicine Education and Telemonitoring on Continuous Positive Airway Pressure Adherence: The Tele-OSA Randomized Trial,” American Journal of Respiratory and Critical Care Medicine, 2018. ZOLL/Respicardia remedē System product information and FDA clearance history.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).