Can a Deviated Septum Cause Sleep Apnea?

If you have been told you have a deviated septum and you also struggle with disrupted sleep, it is reasonable to wonder whether the two are connected. They often travel together, and the relationship between them gets explained badly almost everywhere you look. Some sources imply that straightening your nose will cure your apnea. Others treat the two conditions as completely unrelated. Neither is quite right.
I have lived on the patient side of this question. I had septoplasty to correct a deviated septum years before anyone said the words “sleep apnea” to me, and I was later diagnosed with severe obstructive sleep apnea anyway. So I have a personal stake in getting the answer straight, and I want to walk through what the evidence actually says rather than what sells surgery or sells you on a quick fix. I write as someone who has managed this condition for more than a decade, not as a doctor, so treat everything here as background to bring to a real clinician rather than a substitute for one.
What a deviated septum actually is
Your nasal septum is the wall of bone and cartilage that divides your nose into two passages. In a perfectly built nose it would run straight down the middle and leave two equal channels for air. Very few people are built that way. The large majority of us have some degree of septal deviation, where the wall leans to one side and makes one passage narrower than the other. Most of the time that imbalance causes no trouble at all and people never know they have it.
It becomes a “deviated septum” in the clinical sense when the lean is pronounced enough to cause symptoms. According to the Mayo Clinic, the usual complaints are blockage in one or both nostrils, noisy breathing during sleep, nosebleeds from the dried-out surface of the displaced cartilage, and a tendency to favor sleeping on one side to keep the more open nostril clear. Some people are born with the deviation. For others it follows a nose injury from sport, a fall, or a car accident. Either way, an ENT can usually confirm it in a few minutes with a light and a look inside the nose.
That is worth holding onto before we go further: a deviated septum is a nasal problem. It lives in the nose. As you will see, that detail is the whole key to understanding its real relationship with sleep apnea.
How sleep apnea actually works
To see why the nose is not the center of this story, it helps to be clear on what sleep apnea is in the first place. Sleep apnea is a disorder of repeated breathing pauses during sleep. The pauses can last seconds at a time and repeat dozens or even hundreds of times a night, fragmenting your sleep so badly that you wake up exhausted without ever remembering the interruptions.
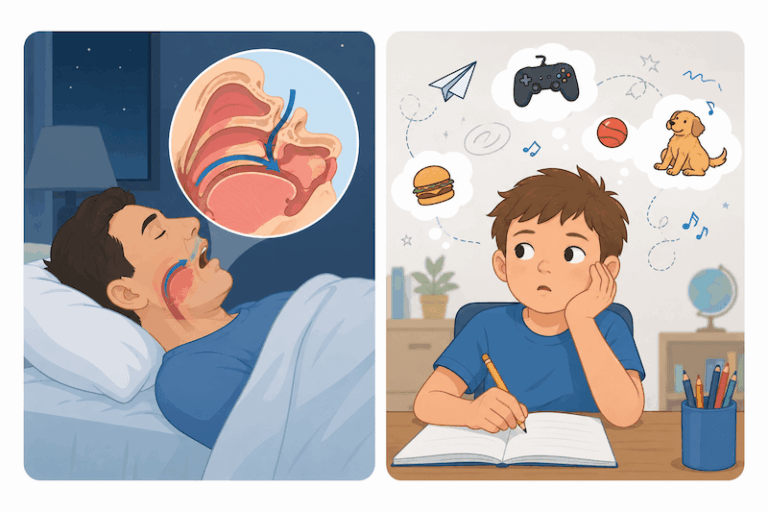
The most common form by far is obstructive sleep apnea, and the defining word there is obstructive. During sleep, the muscles at the back of your throat relax. In people with OSA, they relax too far, and the soft tissue of the throat, the tongue, and the soft palate collapse inward and block the airway. The blockage is at the level of the throat, not the nose. Your brain senses the drop in oxygen, nudges you awake just enough to restore muscle tone and reopen the airway, and the cycle starts over. The symptoms that follow are familiar to anyone who has lived with it: loud snoring, gasping awake, morning headaches, dry mouth, and a flat, foggy tiredness that no amount of coffee fixes.
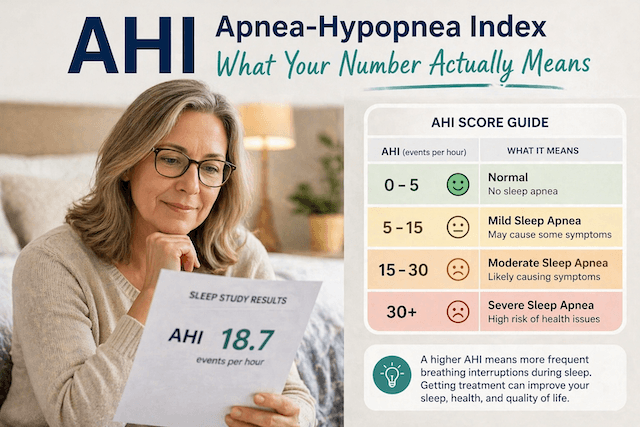
Severity is measured by the apnea-hypopnea index, which counts how many breathing events you have per hour of sleep. Below 5 is normal. From 5 to 15 is mild, 15 to 30 is moderate, and anything above 30 is severe. Keep that scale in mind, because it matters a great deal when we get to the question of whether surgery on your nose can help.
The real connection: an aggravator, not a cause
Here is the part that sources get wrong most often. A deviated septum does not cause obstructive sleep apnea. As the team at SleepApnea.org puts it plainly, a deviated septum cannot create sleep apnea on its own, because the two conditions act in different places. Your septum governs nasal airflow. Your apnea is a collapse in the throat. Straightening the wall in your nose does nothing to stop the throat from collapsing.
What a deviated septum can do is make existing apnea worse, sometimes much worse, and harder to treat. The main route is mouth breathing. When your nasal passages are partly blocked, your body does the only sensible thing and shifts to breathing through your mouth, especially at night when you are not consciously steering your breathing. Mouth breathing changes the geometry of the airway. It lets the jaw drop and the tongue slide back, both of which make the throat more likely to collapse. It also strips away the gentle stabilizing pressure that nasal breathing provides. So a person who already has a throat prone to collapse, and who then adds a blocked nose on top, ends up with apnea that is more frequent, louder, and more stubborn than it would be otherwise.
The cleanest way to picture it is that the throat is the fire and the deviated septum is fuel. The septum did not light the fire. But it can absolutely make it burn hotter. That distinction is not academic. It is the difference between treating your nose and expecting your apnea to vanish, and treating your nose to make your real apnea treatment more bearable.
Can fixing a deviated septum fix sleep apnea?
If the septum is fuel rather than the fire, the honest answer to whether septoplasty cures sleep apnea is mostly no, with a narrow and useful exception.
Septoplasty is the surgery that straightens the septum. A surgeon works inside the nose, repositions or trims the deviated bone and cartilage, and opens up the airflow on the blocked side. It is typically an outpatient procedure, and most people are through the worst of recovery within a couple of weeks. For nasal breathing, it can be genuinely life changing. For apnea itself, the picture is more measured.
The research on nasal surgery for OSA tends to show two things at once. Objectively, in terms of the AHI score, septoplasty alone rarely moves the number much. People who go in with severe apnea generally come out still having severe apnea, because the throat collapse that drives their events was never touched. The clearer benefit shows up at the milder end of the scale and when the nasal blockage was a large part of the overall problem to begin with. Subjectively, though, almost everyone reports feeling better afterward. Sleep feels less broken, daytime sleepiness eases, snoring quiets down, and CPAP becomes far easier to use. That gap between the unchanged number and the improved life tells you something real. Nasal obstruction adds to the burden of disordered breathing in ways that a single hourly count does not fully capture.
So septoplasty is best understood as something that can make your apnea more treatable, not something that treats it. If your apnea is moderate or severe, you should expect to still need a primary therapy such as CPAP, an oral appliance, or in some cases throat level surgery like uvulopalatopharyngoplasty afterward. Clearing the nose simply makes that primary therapy work better.
My own experience with both
I am a useful case study here precisely because my timeline runs in the order that disproves the cure myth. My deviated septum was congenital. I had a noticeably blocked nose for a long time, and breathing freely through it was a daily struggle, so I eventually had septoplasty to correct it. The surgery did exactly what it is supposed to do. My daytime nasal breathing improved a great deal, and I was glad I had it done.
What it did not do was protect me from sleep apnea. Years later I was diagnosed with severe obstructive sleep apnea, with an AHI of 51 at diagnosis. By then my septum was already straight. The apnea showed up anyway, because the apnea was never about my nose. It was about my throat. If a corrected septum could prevent OSA, I would not have it. That single fact reshaped how I think about the whole question.
There is a practical wrinkle to my situation that ties directly back to the mouth breathing point above. I am a chronic mouth breather, which means a nasal mask was never going to work for me, septum or no septum. I use a full face mask that covers the nose and mouth, and that choice was driven by how I breathe rather than by the deviation. So my nose surgery improved my comfort and my daytime life, but my actual apnea is managed entirely by therapy at the throat level, every night.
If you want the longer version of how I got diagnosed and what those first months were like, that story lives over on living with sleep apnea. The short lesson I took from it is that both conditions deserved attention on their own terms, and fixing one did nothing automatic for the other.
Managing both day to day
If you are in the position of having a blocked nose and apnea at the same time, the good part is that the two problems have largely separate, compatible solutions, and addressing the nose tends to make the apnea therapy easier rather than competing with it.
On the nasal side, not everyone needs surgery. Plenty of people get meaningful relief from nasal steroid sprays, short term decongestants used only as directed, antihistamines when allergies are the trigger, or simple nasal strips that hold the outside of the nose open at night. None of these straighten the septum, but they can reduce congestion enough to make breathing and therapy more comfortable. It is worth reading up on the broader menu of alternative approaches as well, with the understanding that they support comfort rather than replace primary apnea treatment.
On the apnea side, CPAP remains the standard for moderate to severe OSA even when a deviated septum is in the picture, but the nose changes how you set it up. A blocked nose is one of the strongest reasons to consider a full face mask over a nasal one, since a full face mask does not depend on clear nasal breathing to deliver pressure. If you are weighing your options, the comparison between a nasal and a full face mask is the first decision to get right, and there is specific guidance on choosing a mask that works around a deviated septum. A heated humidifier is also close to essential, because pressurized air through an already irritated nose can dry it out and make congestion worse without one.
The honest truth about starting CPAP with a blocked nose is that the adjustment period is harder than average. It is doable, but expect it to take patience, and lean on the practical tips for getting used to CPAP therapy rather than white knuckling it. Clearing the nose, whether through surgery or simpler measures, is one of the most reliable ways to make those early weeks easier.
Getting properly evaluated
Because these two conditions overlap in symptoms and feed off each other, the worst approach is to guess. Snoring, daytime exhaustion, and broken sleep can come from either condition or both, and the only way to separate them is to have each one assessed by the right person.
A deviated septum is an ENT’s territory, confirmed with a quick physical look inside the nose. Sleep apnea is diagnosed through a sleep study, either in a lab or with a home sleep test, which is the only way to measure your AHI and learn how severe your apnea really is. If you suspect both, getting both evaluated together is the smart move, because the treatment plan that makes sense depends on how much of your trouble is coming from the nose and how much from the throat. In practice that often means an ENT and a sleep physician comparing notes, which is exactly the kind of two part picture that a single specialist looking at a single organ can miss.
The bottom line
A deviated septum will not cause obstructive sleep apnea, and straightening it will not cure apnea that is already there. The apnea is a collapse in your throat, and your nose is upstream of that. What a deviated septum can do is make your apnea worse by pushing you toward mouth breathing, and make your treatment harder by fighting against a nasal mask and a comfortable night.
That cuts both ways, and the second half is the encouraging part. Clearing the nose, whether with septoplasty or with simpler measures, can make a real difference to how you feel and how well your apnea therapy works, even when it leaves your AHI untouched. My own path is the proof of the limit and the value at once. The surgery fixed my breathing and did nothing for my apnea, and I needed proper therapy for the apnea regardless. If you are dealing with both, treat them as two separate problems that happen to influence each other, get each one assessed properly, and you will end up breathing more freely and sleeping more soundly than chasing either one alone would ever give you.
⚠️ MEDICAL DISCLAIMER This blog provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Sleep apnea is a serious condition, and CPAP equipment should be used under proper medical supervision. Always consult your doctor or sleep specialist before starting, stopping, or changing any therapy. I share personal experiences as a CPAP user, not as a medical professional. Individual results vary. For medical guidance, please consult a qualified clinician or the American Academy of Sleep Medicine (aasm.org).